

Neuro-Inflammation Modulation and Post-Traumatic Brain Injury Lesions: From Bench to Bed-Side
- PMID: 36232495
- PMCID: PMC9570205
- DOI: 10.3390/ijms231911193
Neuro-Inflammation Modulation and Post-Traumatic Brain Injury Lesions: From Bench to Bed-Side
Abstract
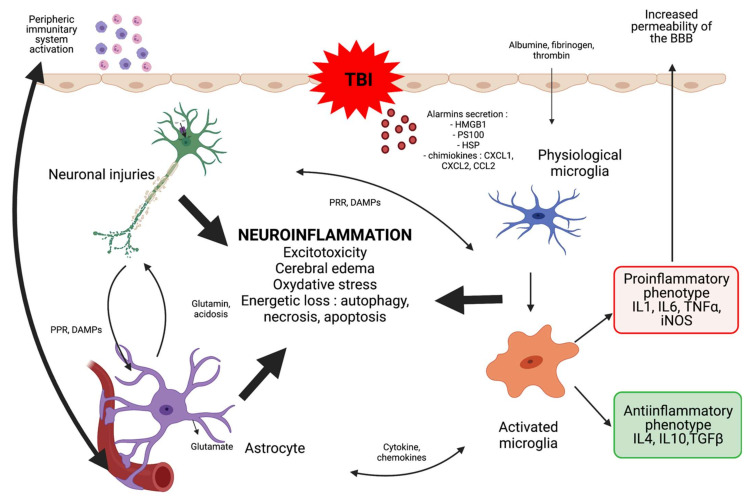
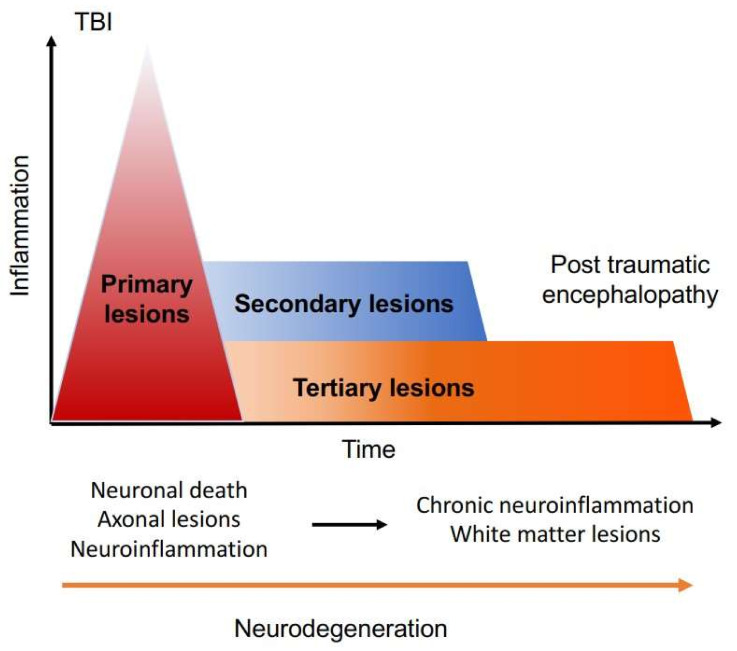
Head trauma is the most common cause of disability in young adults. Known as a silent epidemic, it can cause a mosaic of symptoms, whether neurological (sensory-motor deficits), psychiatric (depressive and anxiety symptoms), or somatic (vertigo, tinnitus, phosphenes). Furthermore, cranial trauma (CT) in children presents several particularities in terms of epidemiology, mechanism, and physiopathology-notably linked to the attack of an immature organ. As in adults, head trauma in children can have lifelong repercussions and can cause social and family isolation, difficulties at school, and, later, socio-professional adversity. Improving management of the pre-hospital and rehabilitation course of these patients reduces secondary morbidity and mortality, but often not without long-term disability. One hypothesized contributor to this process is chronic neuroinflammation, which could accompany primary lesions and facilitate their development into tertiary lesions. Neuroinflammation is a complex process involving different actors such as glial cells (astrocytes, microglia, oligodendrocytes), the permeability of the blood-brain barrier, excitotoxicity, production of oxygen derivatives, cytokine release, tissue damage, and neuronal death. Several studies have investigated the effect of various treatments on the neuroinflammatory response in traumatic brain injury in vitro and in animal and human models. The aim of this review is to examine the various anti-inflammatory therapies that have been implemented.
Keywords: neuroinflammation; neuroprotection; therapeutics; traumatic brain injury.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Menon D.K., Schwab K., Wright D.W., Maas A.I. Demographics and Clinical Assessment Working Group of the International and Interagency Initiative toward Common Data Elements for Research on Traumatic Brain Injury and Psychological Health Position statement: Definition of traumatic brain injury. Arch. Phys. Med. Rehabil. 2010;91:1637–1640. doi: 10.1016/j.apmr.2010.05.017. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
