

Catheter Ablation versus Medical Therapy of Atrial Fibrillation in Patients with Heart Failure: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials
- PMID: 36233407
- PMCID: PMC9572511
- DOI: 10.3390/jcm11195530
Catheter Ablation versus Medical Therapy of Atrial Fibrillation in Patients with Heart Failure: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials
Abstract
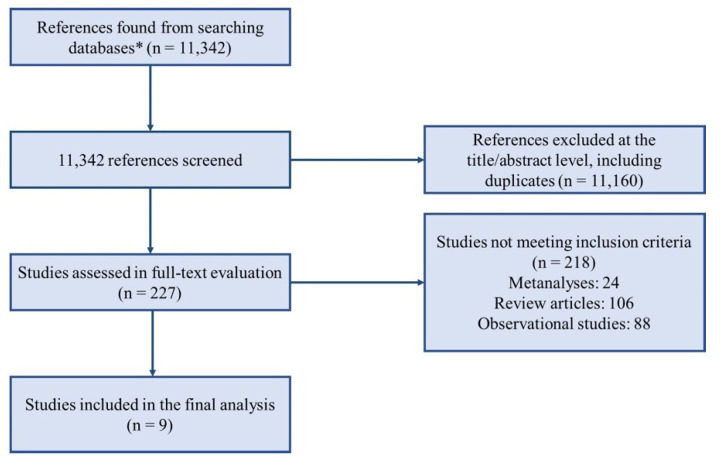
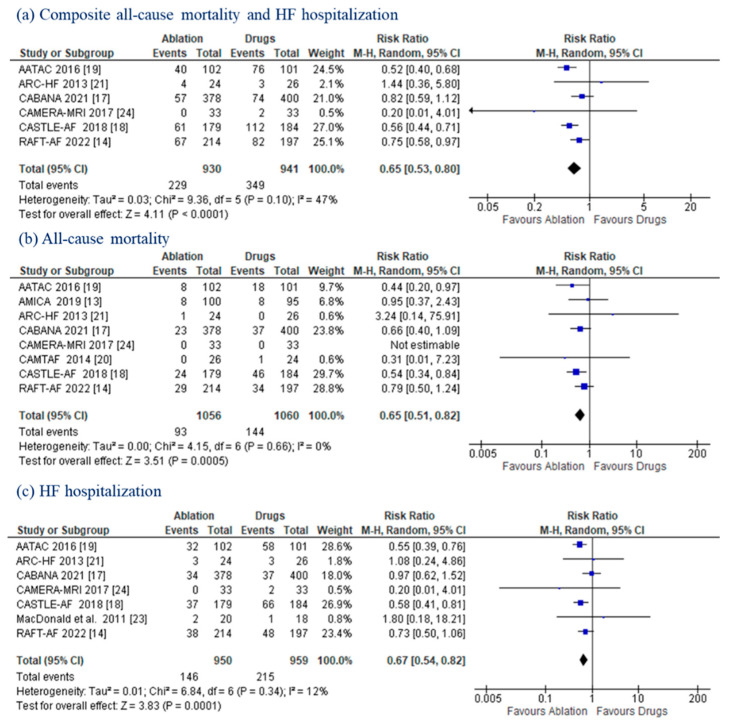
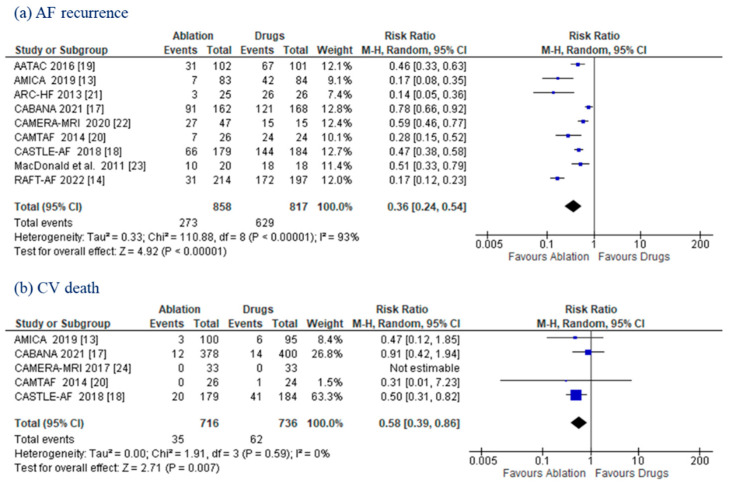
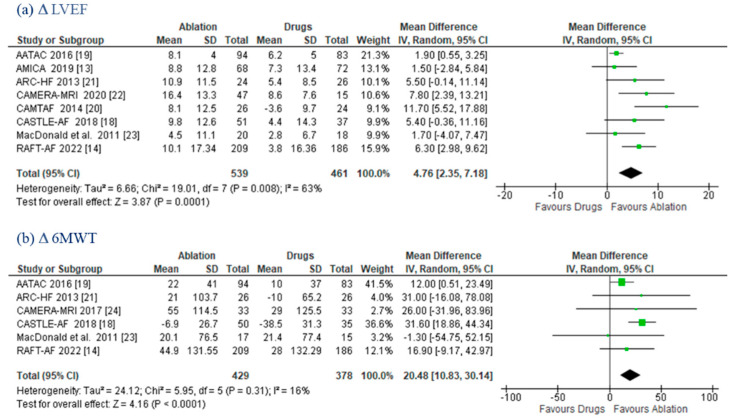
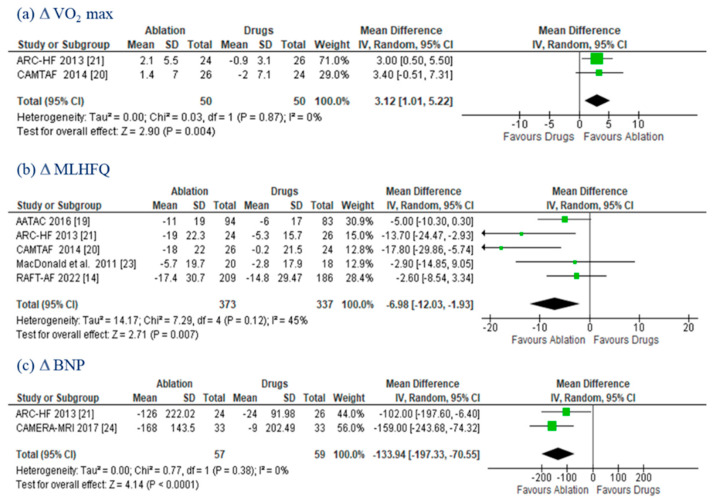
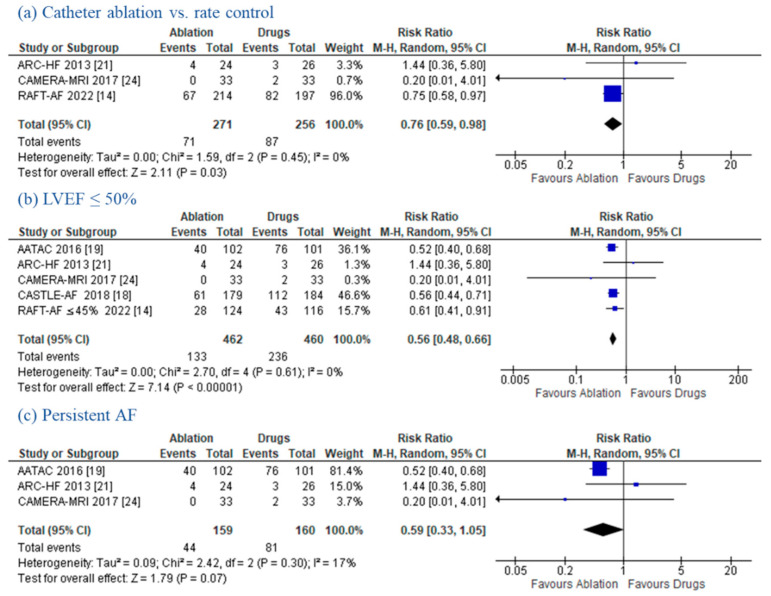
Background: Atrial fibrillation (AF) and heart failure (HF) often coexist and synergistically contribute to an increased risk of hospitalization, stroke, and mortality. Objective: To compare the efficacy of catheter ablation (CA) versus medical therapy (MT) in HF patients with AF. Methods: Electronic databases were queried for randomized controlled trials (RCTs) of CA versus MT of AF in patients with HF. Risk ratios (RRs), mean differences (MDs), and 95% confidence intervals (CIs) were measured using the Mantel−Haenszel method. Results: A total of nine RCTs enrolling 2155 patients met the inclusion criteria. Compared to MT, CA led to a significant reduction in the composite of all-cause mortality and HF hospitalization (24.6% vs. 37.1%; RR: 0.65 (95% CI: 0.53−0.80); p < 0.0001), all-cause mortality (8.8% vs. 13.6%; RR: 0.65 (95% CI: 0.51−0.82); p = 0.0005), HF hospitalization (15.4% vs. 22.4%; (RR: 0.67 (95% CI: 0.54−0.82); p = 0.0001), AF recurrence (31.8% vs. 77.0%; RR: 0.36 (95% CI: 0.24−0.54); p < 0.0001), and cardiovascular (CV) death (4.9% vs. 8.4%; RR: 0.58 (95% CI: 0.39−0.86); p = 0.007). CA improved the left ventricular ejection fraction (MD:4.76% (95% CI: 2.35−7.18); p = 0.0001), 6 min walk test (MD: 20.48 m (95% CI: 10.83−30.14); p < 0.0001), peak oxygen consumption (MD: 3.1 2mL/kg/min (95% CI: 1.01−5.22); p = 0.004), Minnesota Living with Heart Failure Questionnaire score (MD: −6.98 (95% CI: −12−03, −1.93); p = 0.007), and brain natriuretic peptide levels (MD:−133.94 pg/mL (95% CI: −197.33, −70.55); p < 0.0001). Conclusions: In HF patients, AF catheter ablation was superior to MT in reducing CV and all-cause mortality. Further significant benefits occurred within the ablation group in terms of HF hospitalizations, AF recurrences, the systolic function, exercise capacity, and quality of life.
Keywords: atrial fibrillation; catheter ablation; heart failure; medical therapy; randomized controlled trials; recurrence.
Conflict of interest statement
Dr. Chierchia received compensation for teaching purposes and proctoring from Medtronic, Abbott, Biotronik, Boston Scientific, and Acutus Medical. Dr. de Asmundis receives research grants on behalf of the center from Biotronik, Medtronic, Abbott, LivaNova, Boston Scientific, AtriCure, Philips, and Acutus, and compensation for teaching purposes and proctoring from Medtronic, Abbott, Biotronik, Livanova, Boston Scientific, Atricure, Acutus Medical, and Daiichi Sankyo. Dr. Di Biase is a consultant for Biosense Webster, Boston Scientific, Stereotaxis, and St. Jude Medical. Dr. Di Biase received speaker honoraria/travel support grants from Medtronic, Bristol Meyers Squibb, Pfizer, and Biotronik. Dr. Natale has received speaker honoraria from Boston Scientific, Biosense Webster, St. Jude Medical, Biotronik, and Medtronic, and is a consultant for Biosense Webster, St. Jude Medical, and Janssen. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Similar articles
-
Efficacy of catheter ablation for atrial fibrillation in heart failure: a meta-analysis of randomized controlled trials.ESC Heart Fail. 2024 Oct;11(5):2684-2693. doi: 10.1002/ehf2.14814. Epub 2024 Apr 25. ESC Heart Fail. 2024. PMID: 38661235 Free PMC article.
-
Catheter ablation for treatment of patients with atrial fibrillation and heart failure: a meta-analysis of randomized controlled trials.BMC Cardiovasc Disord. 2018 Aug 13;18(1):165. doi: 10.1186/s12872-018-0904-3. BMC Cardiovasc Disord. 2018. PMID: 30103676 Free PMC article. Review.
-
Catheter Ablation of Atrial Fibrillation in Patients With Heart Failure: A Meta-analysis of Randomized Controlled Trials.Ann Intern Med. 2019 Jan 1;170(1):41-50. doi: 10.7326/M18-0992. Epub 2018 Dec 25. Ann Intern Med. 2019. PMID: 30583296
-
Catheter ablation for atrial fibrillation in heart failure with reduced ejection fraction patients: A meta-analysis.Heart Rhythm. 2024 Sep;21(9):1604-1612. doi: 10.1016/j.hrthm.2024.04.098. Epub 2024 May 3. Heart Rhythm. 2024. PMID: 38705438
-
Prognostic benefit of catheter ablation of atrial fibrillation in heart failure: An updated meta-analysis of randomized controlled trials.J Arrhythm. 2023 Jan 17;39(2):129-141. doi: 10.1002/joa3.12812. eCollection 2023 Apr. J Arrhythm. 2023. PMID: 37021020 Free PMC article.
Cited by
-
Value of Imaging in the Non-Invasive Prediction of Recurrence after Catheter Ablation in Patients with Atrial Fibrillation: An Up-to-Date Review.Rev Cardiovasc Med. 2023 Aug 18;24(8):241. doi: 10.31083/j.rcm2408241. eCollection 2023 Aug. Rev Cardiovasc Med. 2023. PMID: 39076720 Free PMC article. Review.
-
Catheter ablation in patients with paroxysmal atrial fibrillation and absence of structural heart disease: A meta-analysis of randomized trials.Int J Cardiol Heart Vasc. 2023 Nov 5;49:101292. doi: 10.1016/j.ijcha.2023.101292. eCollection 2023 Dec. Int J Cardiol Heart Vasc. 2023. PMID: 38020055 Free PMC article.
-
Atrial fibrillation in heart failure: drugs or ablation?Eur Heart J Suppl. 2023 Apr 21;25(Suppl B):B28-B30. doi: 10.1093/eurheartjsupp/suad063. eCollection 2023 Apr. Eur Heart J Suppl. 2023. PMID: 37091661 Free PMC article.
-
2023 National Heart Center/Saudi Heart Association Focused Update of the 2019 Saudi Heart Association Guidelines for the Management of Heart Failure.J Saudi Heart Assoc. 2023 May 25;35(1):71-134. doi: 10.37616/2212-5043.1334. eCollection 2023. J Saudi Heart Assoc. 2023. PMID: 37323135 Free PMC article.
-
Assessment of Redundant Meta-Analyses on Catheter Ablation of Atrial Fibrillation in Patients with Heart Failure.Rev Cardiovasc Med. 2024 Nov 21;25(11):418. doi: 10.31083/j.rcm2511418. eCollection 2024 Nov. Rev Cardiovasc Med. 2024. PMID: 39618855 Free PMC article.
References
-
- Sanders P., Morton J.B., Davidson N.C., Spence S.J., Vohra J.K., Sparks P.B., Kalman J.M. Electrical remodeling of the atria in congestive heart failure: Electrophysiological and electroanatomic mapping in humans. Circulation. 2003;108:1461–1468. doi: 10.1161/01.CIR.0000090688.49283.67. - DOI - PubMed
-
- Della Rocca D.G., Santini L., Forleo G.B., Sanniti A., Del Prete A., Lavalle C., Di Biase L., Natale A., Romeo F. Novel Perspectives on Arrhythmia-Induced Cardiomyopathy: Pathophysiology, Clinical Manifestations and an Update on Invasive Management Strategies. Cardiol. Rev. 2015;23:135–141. doi: 10.1097/CRD.0000000000000040. - DOI - PubMed
-
- Della Rocca D.G., Tarantino N., Trivedi C., Mohanty S., Anannab A., Salwan A.S., Gianni C., Bassiouny M., Al-Ahmad A., Romero J., et al. Non-pulmonary vein triggers in nonparoxysmal atrial fibrillation: Implications of pathophysiology for catheter ablation. J. Cardiovasc. Electrophysiol. 2020;31:2154–2167. doi: 10.1111/jce.14638. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
