Systematic Review and Meta-Analysis of Pleurectomy/Decortication versus Extrapleural Pneumonectomy in the Treatment of Malignant Pleural Mesothelioma
- PMID: 36233416
- PMCID: PMC9571799
- DOI: 10.3390/jcm11195544
Systematic Review and Meta-Analysis of Pleurectomy/Decortication versus Extrapleural Pneumonectomy in the Treatment of Malignant Pleural Mesothelioma
Abstract
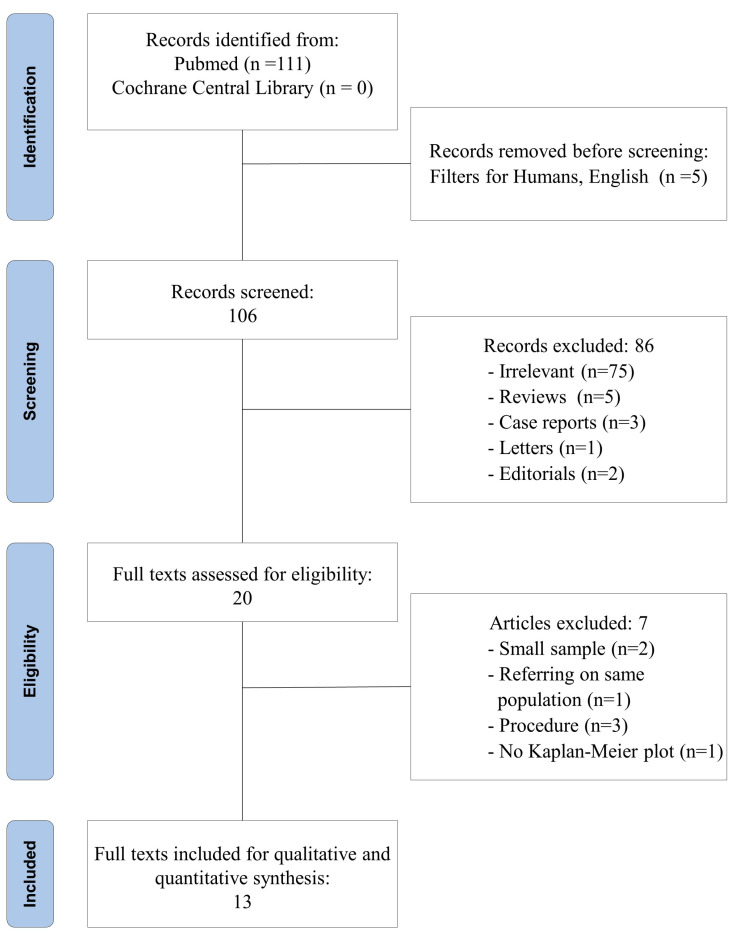
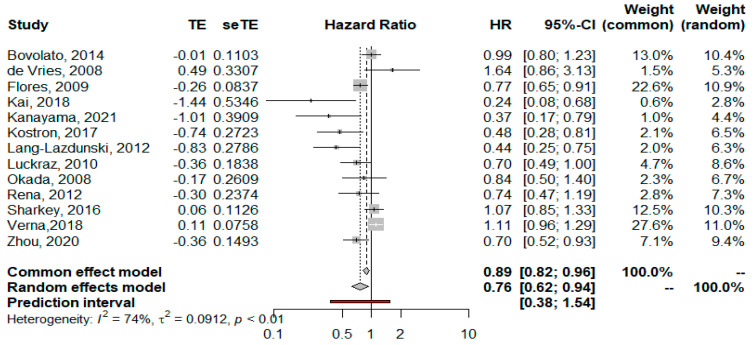
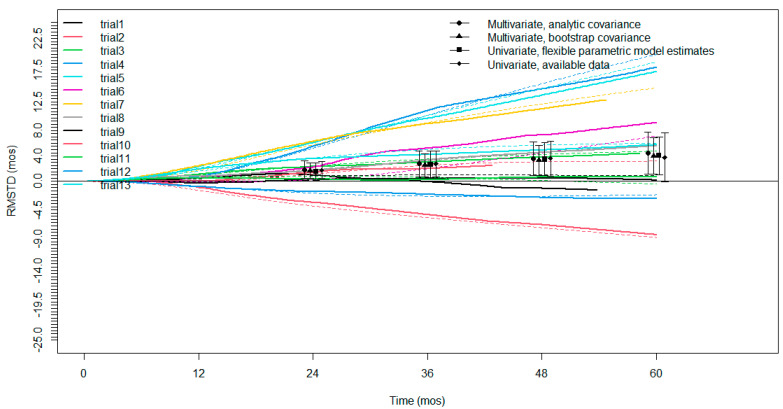
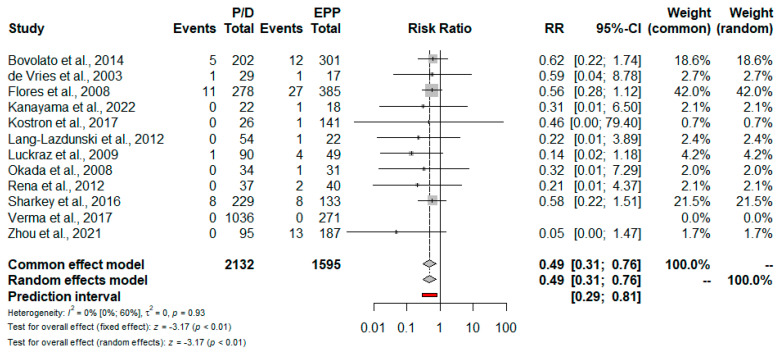
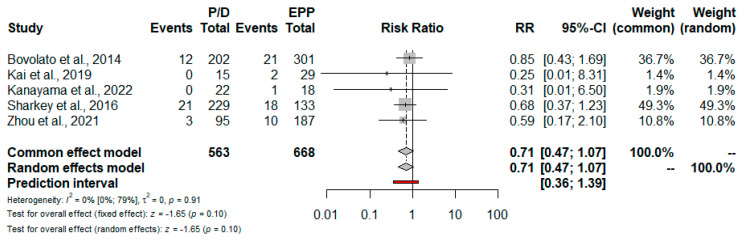
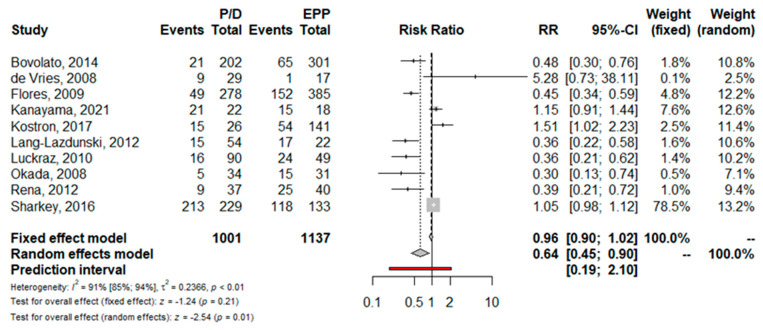
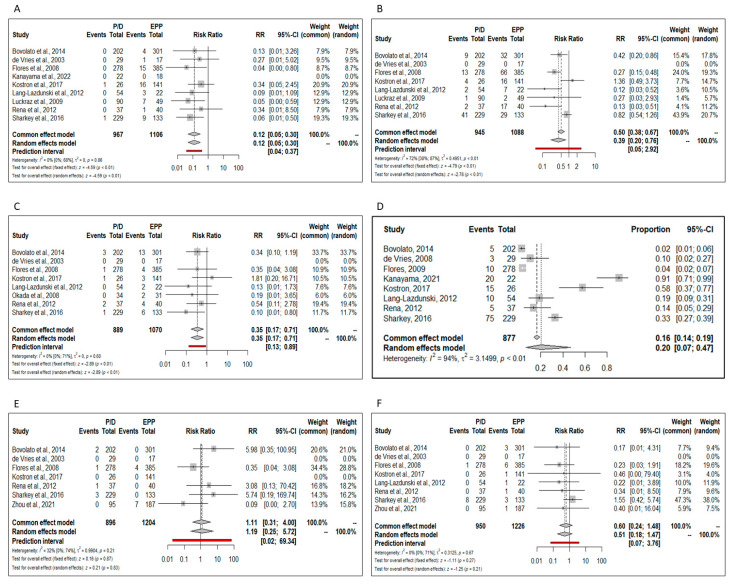
Objective: Malignant pleural mesothelioma (MPM) is a rare and aggressive malignant cancer for which there are poor treatment options. Extrapleural pneumonectomy (EPP) and pleurectomy decortication (P/D) are the two most used surgical procedures in patients with resectable disease. We reviewed the available literature in order to compare the overall survival and postoperative complications of EPP and P/D and to provide evidence for the best procedure in the treatment of MPM. Methods: We performed a systematic review of the literature, including studies from August 2018 to May 2022. The primary outcome was 5-year overall survival (OS) and the secondary outcomes were 30-day mortality, 90-day mortality and peri-operative complications. Results: Thirteen studies were considered, including a total of 1624 patients treated with EPP and 2147 treated with P/D. The estimated pooled HR showed a significant lower hazard for P/D compared to EPP in terms of OS (HR = 0.76; 95% CI from 0.62 to 0.94; p < 0.001). In 12 studies, the risk for 30-day mortality was lower for patients treated with P/D (RR = 0.49; 95% CI from 0.31 to 0.76; p = <0.01), whereas only five studies reported 90-day mortality, and no statistically significant difference between EPP and P/D was found (RR = 0.71; 95% CI from 0.47 to 1.07; p = 0.10). The OS restricted mean survival time difference meta-analysis (RMSDT) confirms the superior survival of P/D on the EPP, a superiority that increases from 0.54 months at one year to 4.23 at five years. The incidence of postoperative empyema, atrial fibrillation, bleeding and bronchopleural fistula was significantly increased in the EPP group except for prolonged air leakage, which is only characteristic of P/D. Conclusions: Using two different statistical methods, this meta-analysis suggests that long-term survival after surgical treatment for resectable MPM is greater for patients undergoing P/D. Long-term survival had never been previously analyzed with appropriate tests; on the contrary, our result is consistent with the previous meta-analyses and reinforces the evidence of lower 30-day mortality and the prevalence of postoperative complications in P/D versus EPP patients. The recent introduction of innovative therapeutic schemes, both adjuvant and neoadjuvant therapy, keeps the discussion on surgical strategy open and will require new studies.
Keywords: EPP; malignant pleural mesothelioma; mesothelioma; mpm; pleurectomy; pleurectomy/decortication (P/D); pneumonectomy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures