

Subcapsular Liver Hematoma-A Life-Threatening Condition in Preterm Neonates-A Case Series and Systematic Review of the Literature
- PMID: 36233552
- PMCID: PMC9571888
- DOI: 10.3390/jcm11195684
Subcapsular Liver Hematoma-A Life-Threatening Condition in Preterm Neonates-A Case Series and Systematic Review of the Literature
Abstract
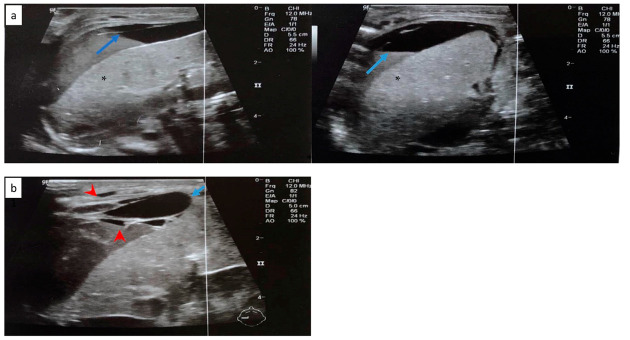
The subcapsular hematoma (SLH) of the liver is a rare finding in living infants. The clinical presentation of rupture is non-specific, with the signs of hypovolemic shock dominating. The causes are several, with prematurity, trauma and sepsis playing a leading role in the creation of an SHL. Umbilical vein catheterization and an increased bleeding tendency have also been associated with this usually fatal diagnosis. Abdominal ultrasonography, among other imaging methods, comprises the gold standard examination for early diagnosis. It should be differentiated from other possible causes of shock, such as sepsis and intraventricular hemorrhage, which have similar clinical presentation. We report a case series of three very low birth weight preterms (VLBW), with an SHL, during the first days of life, one of which survived from this usually catastrophic condition. A comprehensive review of the literature regarding this clinical entity was also conducted. A high index of suspicion is essential for early identification of such a case, with conservative or surgical treatment being the way to go.
Keywords: neonates; preterm neonates; subcapsular liver hematoma; very-low-birth-weight.
Conflict of interest statement
The authors declare no conflict of interest.
Figures








References
Publication types
LinkOut - more resources
Full Text Sources
