

Adherence to the Mediterranean Diet Is Associated with a More Favorable Left Ventricular Geometry in Patients with End-Stage Kidney Disease
- PMID: 36233612
- PMCID: PMC9571193
- DOI: 10.3390/jcm11195746
Adherence to the Mediterranean Diet Is Associated with a More Favorable Left Ventricular Geometry in Patients with End-Stage Kidney Disease
Abstract
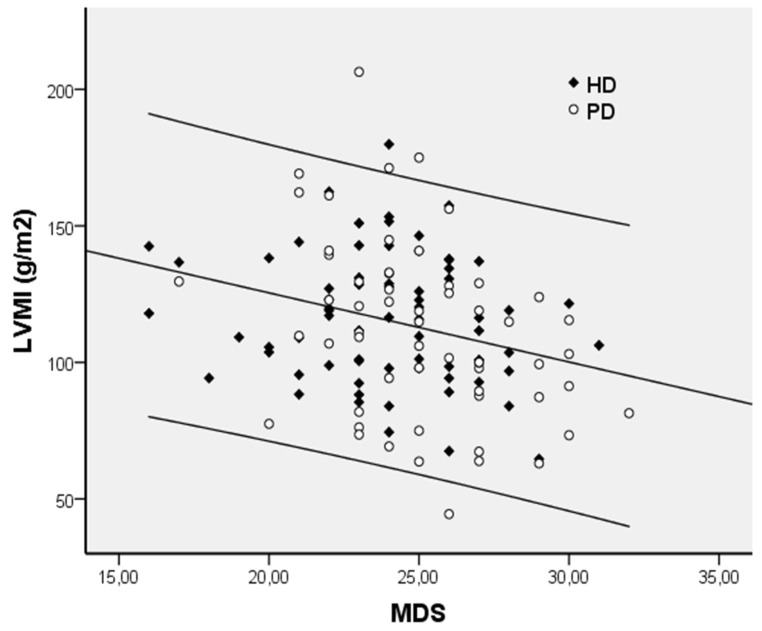
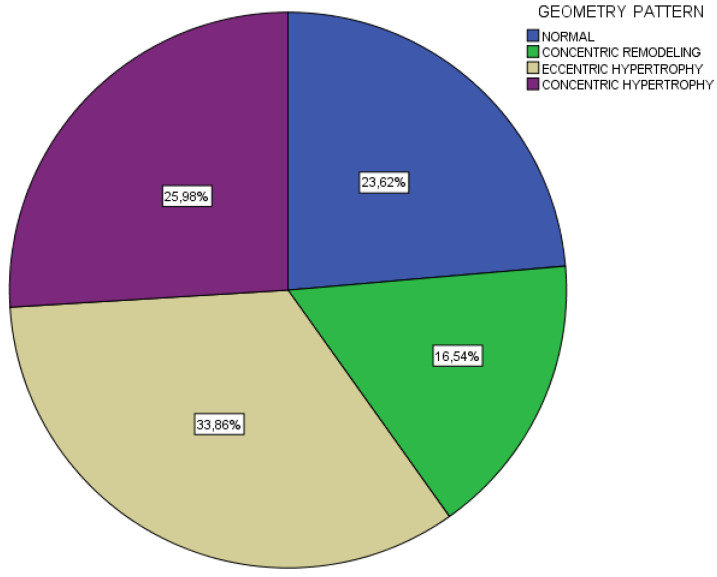
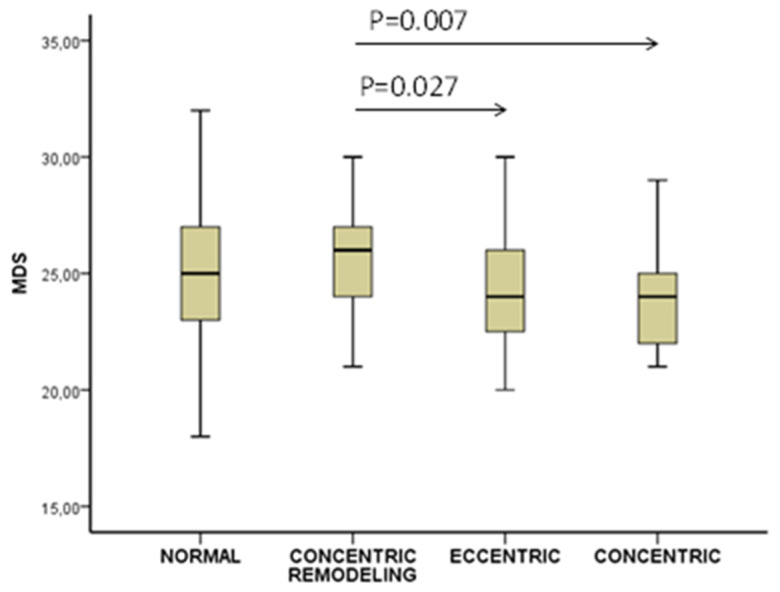
Introduction. The aim of the study was to examine the impact of adherence to a Mediterranean-style diet (MD) on left ventricular hypertrophy (LVH) and cardiac geometry in chronic kidney disease patients on dialysis (CKD-5D), given the high prevalence of cardiovascular morbidity in this population. Methods. n = 127 (77 men and 50 women) CKD-5D patients (69 on hemodialysis and 58 on peritoneal dialysis) with a mean age of 62 ± 15 years were studied. An MD adherence score (MDS) (range 0−55, 55 representing maximal adherence) was estimated with a validated method. Echocardiographic LVH was defined by LV mass index (LVMI) > 95 g/m2 in women and >115 g/m2 in men. Based on LVMI and relative wall thickness (RWT), four LV geometric patterns were defined: normal (normal LVMI and RWT), concentric remodeling (normal LVMI and increased RWT > 0.42), eccentric LVH (increased LVMI and normal RWT), and concentric LVH (increased LVMI and RWT). Results. Patients with LVH (n = 81) as compared to patients with no LVH (n = 46) were older in age (66 ± 13 vs. 55 ± 16 years; p < 0.001) had lower MDS (24 ± 2.7 vs. 25 ± 4.3; p < 0.05) and higher malnutrition-inflammation score (5.0 ± 2.7 vs. 3.9 ± 1.9; p < 0.05), body mass index (27.5 ± 4.9 vs. 24.1 ± 3.5 kg/m2; p < 0.001), prevalence of diabetes (79% vs. 20%; p < 0.05), coronary artery disease (78% vs. 20%; p < 0.05) and peripheral vascular disease (78% vs. 20%; p < 0.01). In a multivariate logistic regression analysis adjusted for all factors mentioned above, each 1-point greater MDS was associated with 18% lower odds of having LVH (OR = 0.82, 95% CI: 0.69−0.98; p < 0.05). MDS was inversely related to LVMI (r = −0.273; p = 0.02), and in a multiple linear regression model (where LVMI was analyzed as a continuous variable), MDS emerged as a significant (Β = −2.217; p < 0.01) independent predictor of LVH. Considering LV geometry, there was a progressive decrease in MDS from the normal group (25.0 ± 3.7) to concentric remodeling (25.8 ± 3.0), eccentric (24.0 ± 2.8), and then concentric (23.6 ± 2.7) group (p < 0.05 for the trend). Conclusions. The greater adherence to an MD is associated with lesser LVH, an important cardiovascular disease risk factor; MD preserves normal cardiac geometry and may confer protection against future cardiac dysfunction in dialysis patients.
Keywords: Mediterranean diet; cardiac geometry; end-stage kidney disease; left ventricular hypertrophy.
Conflict of interest statement
The authors declare that they have no competing interest.
Figures
References
-
- Staplin N., Haynes R., Herrington W.G., Reith C., Cass A., Fellström B., Jiang L., Kasiske B.L., Krane V., Levin A., et al. Smoking and Adverse Outcomes in Patients With CKD: The Study of Heart and Renal Protection (SHARP) Am. J. Kidney Dis. 2016;68:371–380. doi: 10.1053/j.ajkd.2016.02.052. - DOI - PMC - PubMed
-
- Prospective Studies Collaboration. Whitlock G., Lewington S., Sherliker P., Clarke R., Emberson J., Halsey J., Qizilbash N., Collins R., Peto R. Body-mass index and cause-specific mortality in 900,000 adults: Collaborative analyses of 57 prospective studies. Lancet. 2009;373:1083–1096. doi: 10.1016/s0140-6736(09)60318-4. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
