

Risk-Benefit Balance of Renin-Angiotensin-Aldosterone Inhibitor Cessation in Heart Failure Patients with Hyperkalemia
- PMID: 36233692
- PMCID: PMC9572691
- DOI: 10.3390/jcm11195828
Risk-Benefit Balance of Renin-Angiotensin-Aldosterone Inhibitor Cessation in Heart Failure Patients with Hyperkalemia
Erratum in
-
Correction: Kohsaka et al. Risk-Benefit Balance of Renin-Angiotensin-Aldosterone Inhibitor Cessation in Heart Failure Patients with Hyperkalemia. J. Clin. Med. 2022, 11, 5828.J Clin Med. 2023 Mar 29;12(7):2578. doi: 10.3390/jcm12072578. J Clin Med. 2023. PMID: 37048834 Free PMC article.
Abstract
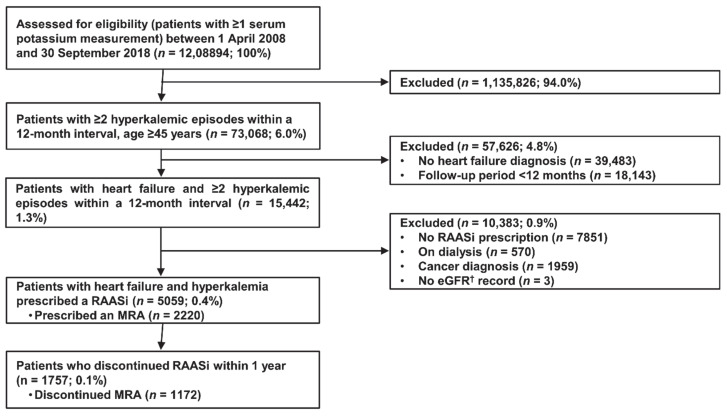
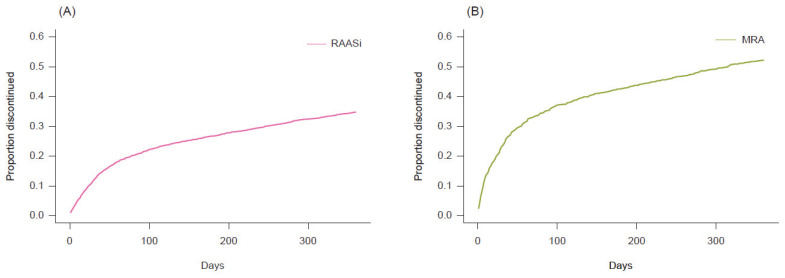
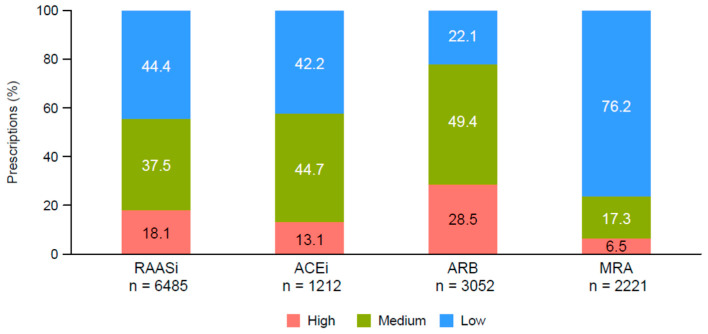
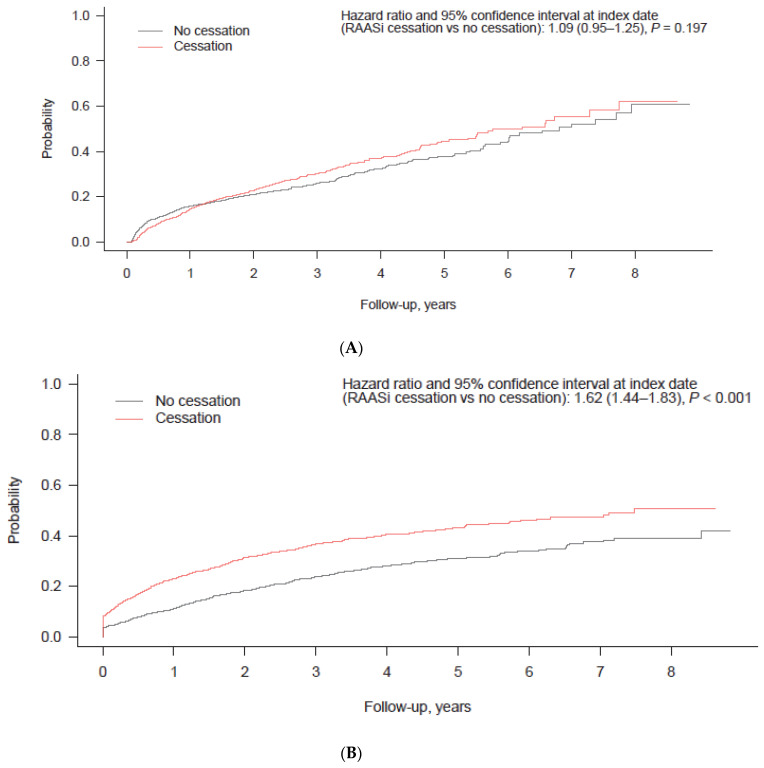
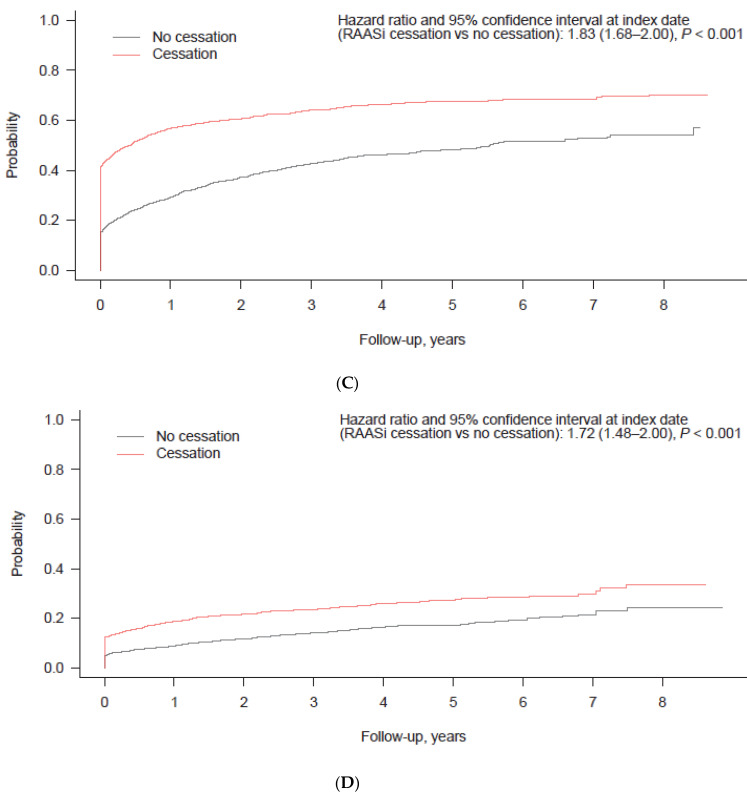
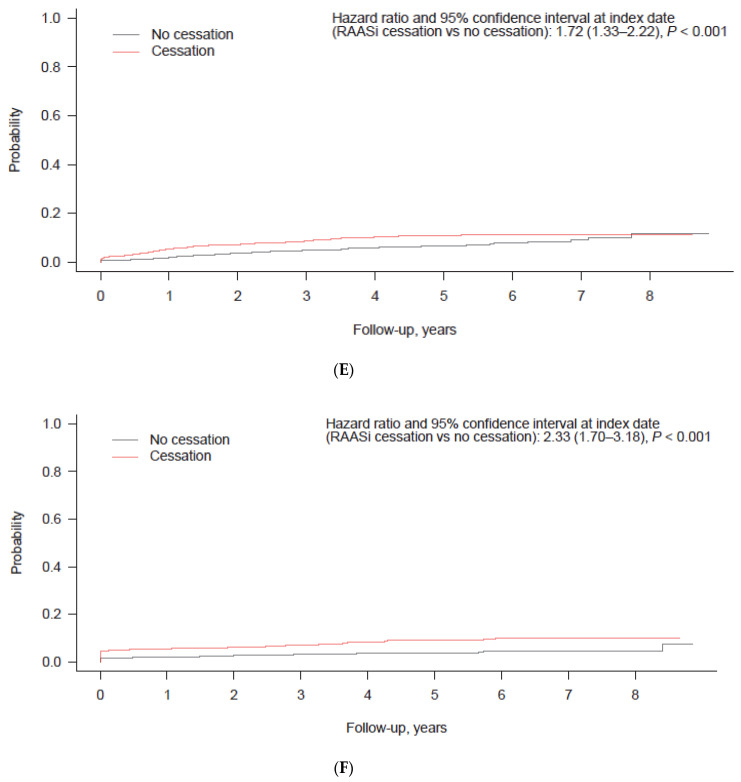
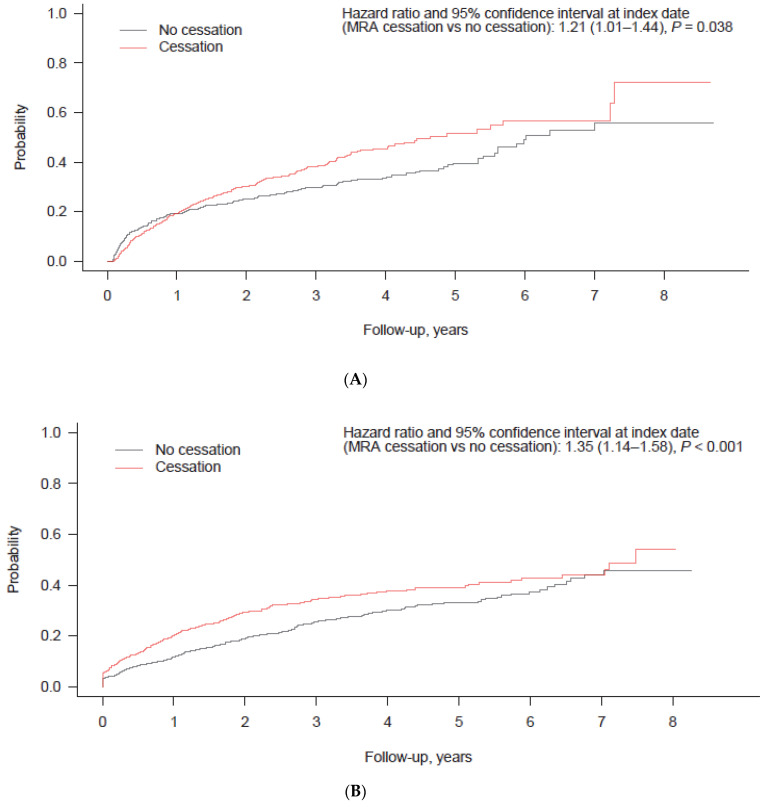
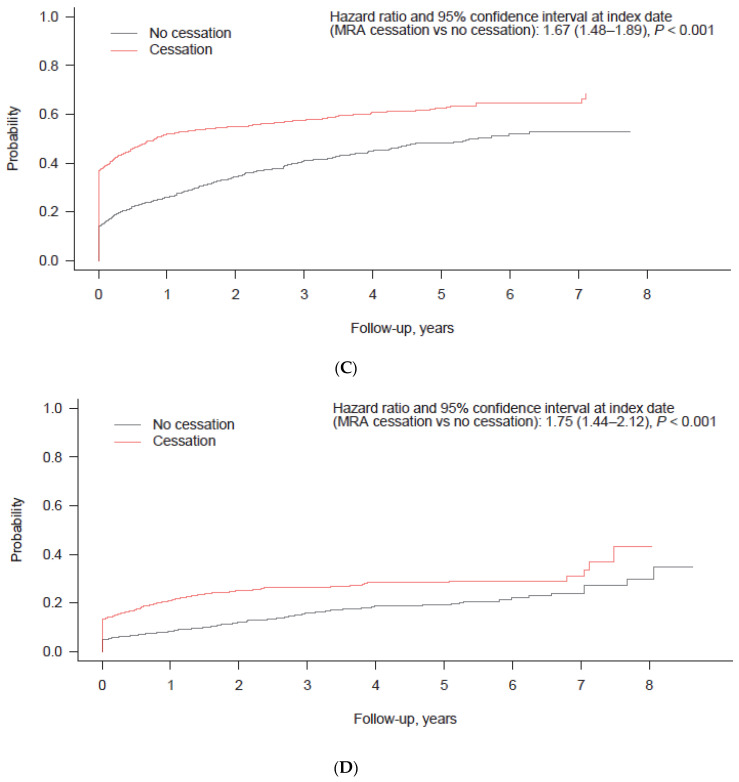
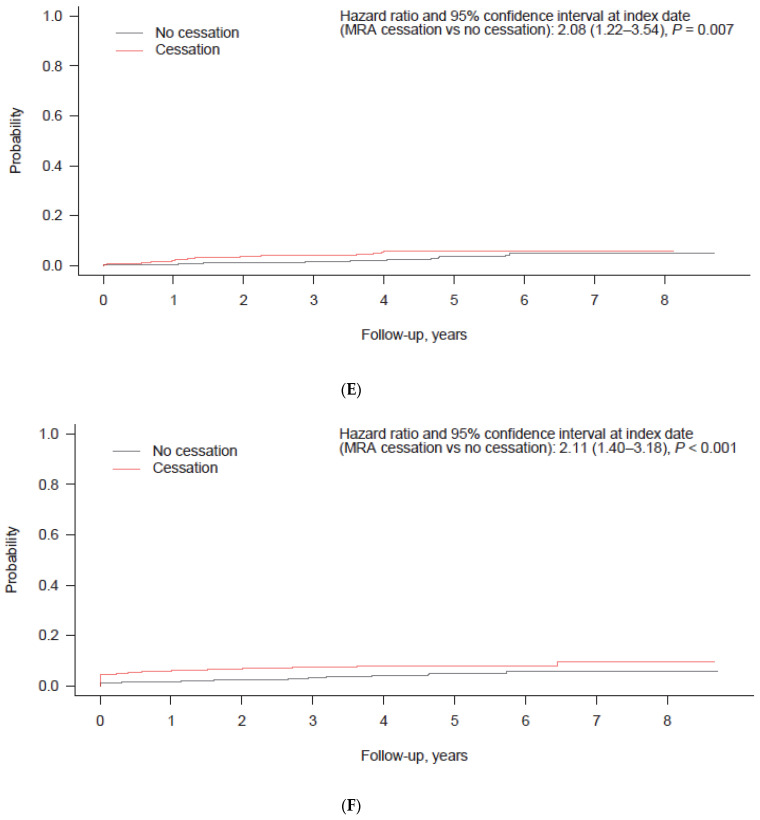
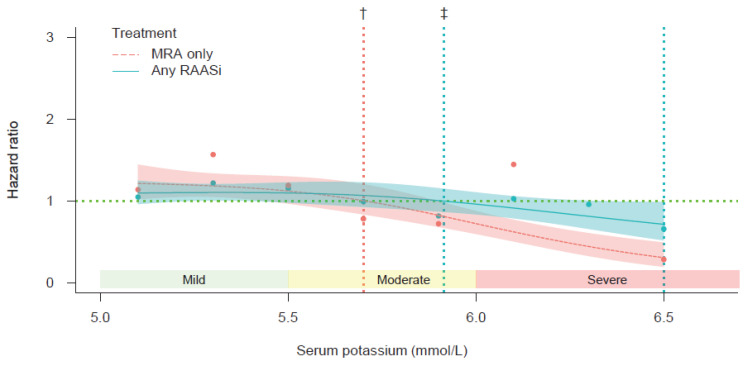
Background: Whether to continue renin−angiotensin−aldosterone system inhibitor (RAASi) therapy in patients with hyperkalemia remains a clinical challenge, particularly in patients with heart failure (HF), where RAASis remain the cornerstone of treatment. We investigated the incidence of dose reduction or the cessation of RAASis and evaluated the threshold of serum potassium at which cessation alters the risk−benefit balance. Methods: This retrospective analysis of a Japanese nationwide claims database investigated treatment patterns of RAASis over 12 months after the initial hyperkalemic episode. The incidences of the clinical outcomes of patients with RAASi (all ACEi/ARB/MRA) or MRA-only cessation (vs. non-cessation) were compared via propensity score-matched patients. A cubic spline regression analysis assessed the hazard of death resulting from treatment cessation vs. no cessation at each potassium level. Results: A total of 5059 hyperkalemic HF patients were identified; most received low to moderate doses of ACEis and ARBs (86.9% and 71.5%, respectively) and low doses of MRAs (76.2%). The RAASi and MRA cessation rates were 34.7% and 52.8% at 1 year post-diagnosis, while the dose reduction rates were 8.4% and 6.5%, respectively. During the mean follow-up of 2.8 years, patients who ceased RAASi or MRA therapies were at higher risk for adverse outcomes; cubic spline analysis found that serum potassium levels of <5.9 and <5.7 mmol/L conferred an increased mortality risk for RAASi and MRA cessation, respectively. Conclusions: Treatment cessation/dose reduction of RAASis are common among HF patients. The risks of RAASi/MRA cessation may outweigh the benefits in patients with mild to moderate hyperkalemia.
Keywords: heart failure; hyperkalemia; mineralocorticoid receptor antagonists; renin–angiotensin–aldosterone system inhibitors; risk–benefit.
Conflict of interest statement
S.K. reports investigator-initiated grant funding from Daiichi Sankyo and personal fees from AstraZeneca, Bayer, Bristol-Myers Squibb, and Pfizer. S.O., N.M., and T.Y. are employees of AstraZeneca K.K.
Figures
References
-
- Oliveros E., Oni E.T., Shahzad A., Kluger A.Y., Lo K.B., Rangaswami J., McCullough P.A. Benefits and risks of continuing angiotensin-converting enzyme inhibitors, angiotensin II receptor antagonists, and mineralocorticoid receptor antagonists during hospitalizations for acute heart failure. Cardiorenal Med. 2020;10:69–84. doi: 10.1159/000504167. - DOI - PubMed
-
- Rosano G.M.C., Tamargo J., Kjeldsen K.P., Lainscak M., Agewall S., Anker S.D., Ceconi C., Coats A.J.S., Drexel H., Filippatos G., et al. Expert consensus document on the management of hyperkalaemia in patients with cardiovascular disease treated with renin angiotensin aldosterone system inhibitors: Coordinated by the Working Group on Cardiovascular Pharmacotherapy of the European Society of Cardiology. Eur. Heart J. Cardiovasc. Pharmacother. 2018;4:180–188. - PubMed
-
- Xie X., Liu Y., Perkovic V., Xiangling L., Ninomiya T., Hou W., Zhao N., Liu L., Lv J., Zhang H., et al. Renin-angiotensin system inhibitors and kidney and cardiovascular outcomes in patients with CKD: A Bayesian network meta-analysis of randomized clinical trials. Am. J. Kidney Dis. 2016;67:728–741. doi: 10.1053/j.ajkd.2015.10.011. - DOI - PubMed
-
- Heidenreich P.A., Bozkurt B., Aguilar D., Allen L.A., Byun J.J., Colvin M.M., Deswal A., Drazner M.H., Dunlay S.M., Evers L.R., et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022;79:e263–e421. doi: 10.1016/j.jacc.2021.12.012. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
