

Sex-Related Differences in Clinical Outcomes in Patients with Atrial Fibrillation and Coronary Artery Disease: A Sub-Study of the MISOAC-AF Randomized Controlled Trial
- PMID: 36233711
- PMCID: PMC9571749
- DOI: 10.3390/jcm11195843
Sex-Related Differences in Clinical Outcomes in Patients with Atrial Fibrillation and Coronary Artery Disease: A Sub-Study of the MISOAC-AF Randomized Controlled Trial
Abstract
Background: There is limited "real-world" data on the prognostic role of gender in comorbid atrial fibrillation (AF) and coronary artery disease (CAD).
Methods: In this post-hoc analysis of the MISOAC-AF randomized trial (NCT: 02941978), consecutive patients with AF and CAD who were discharged from the cardiology ward between 2015 and 2018 were included. Multivariable Cox-regression analysis was performed for all-cause mortality and cardiovascular (CV) mortality. Competing-risk analysis was performed for the outcomes of stroke or systemic embolism, major bleeding, AF- or heart failure (HF)-related hospitalization, adjusted for the competing risk of all-cause death.
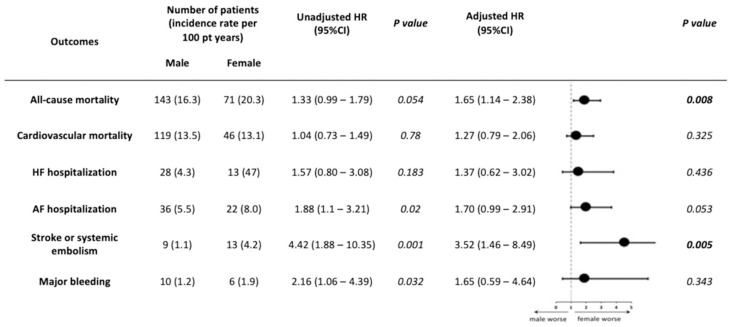
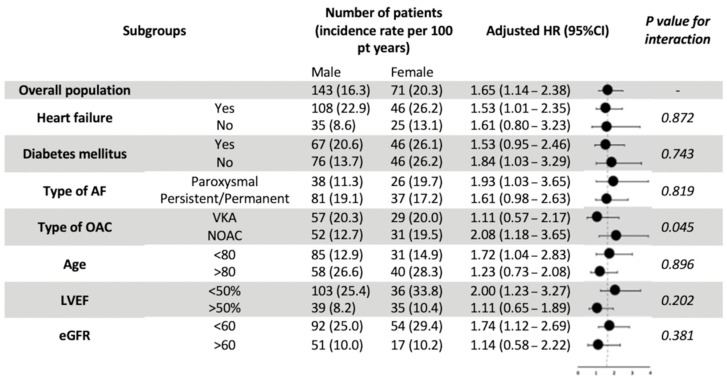
Results: Of 1098 patients with AF, 461 patients with comorbid CAD were analyzed. Women were older and more likely to have a history of diabetes mellitus and valvular heart disease, while men were more likely to have a history of smoking or myocardial infarction. Over a median follow-up of 31 months, 143 (43.4%) men and 71 (53.7%) women died. Women were at a higher risk for all-cause mortality (adjusted hazard ration [aHR] 1.65; 95% confidence interval [CI] 1.14-2.38) and stroke or systemic embolism (aHR 3.52; 95% CI 1.46-8.49) compared to men. The risks of CV mortality, major bleeding, AF-related hospitalization, and HF-related hospitalization were similar between genders.
Conclusions: In recently hospitalized patients with AF and comorbid CAD, the female gender was independently associated with increased all-cause mortality and thromboembolic events.
Keywords: atrial fibrillation; coronary artery disease; prognosis; sex.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Associations of Atrial Fibrillation Patterns With Mortality and Cardiovascular Events: Implications of the MISOAC-AF Trial.J Cardiovasc Pharmacol Ther. 2022 Jan-Dec;27:10742484211069422. doi: 10.1177/10742484211069422. J Cardiovasc Pharmacol Ther. 2022. PMID: 35006026
-
Prognostic significance of diabetes mellitus in patients with atrial fibrillation.Cardiovasc Diabetol. 2021 Feb 11;20(1):40. doi: 10.1186/s12933-021-01232-7. Cardiovasc Diabetol. 2021. PMID: 33573666 Free PMC article.
-
Association of Length of Stay With the Clinical Trajectory of Hospitalized Patients With Atrial Fibrillation: Staying Less Is More?Am J Cardiol. 2023 Nov 1;206:254-261. doi: 10.1016/j.amjcard.2023.08.066. Epub 2023 Sep 14. Am J Cardiol. 2023. PMID: 37716224
-
Prognostic implications of atrial fibrillation in patients with stable coronary artery disease: a systematic review and meta-analysis of adjusted observational studies.Rev Cardiovasc Med. 2021 Jun 30;22(2):439-444. doi: 10.31083/j.rcm2202049. Rev Cardiovasc Med. 2021. PMID: 34258910
-
Direct Oral Anticoagulants vs. Warfarin in Latin American Patients With Atrial Fibrillation: Evidence From Four post-hoc Analyses of Randomized Clinical Trials.Front Cardiovasc Med. 2022 Mar 4;9:841341. doi: 10.3389/fcvm.2022.841341. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35310968 Free PMC article.
Cited by
-
Ethnic and Gender Variations in Ischemic Stroke Patterns among Arab Populations in Northern Israel: A Preliminary Exploration towards Culturally Aware Personalized Stroke Care.J Pers Med. 2024 May 15;14(5):526. doi: 10.3390/jpm14050526. J Pers Med. 2024. PMID: 38793108 Free PMC article.
References
-
- Van Gelder I.C., Groenveld H.F., Crijns H.J.G.M., Tuininga Y.S., Tijssen J.G.P., Alings A.M., Hillege H.L., Bergsma-Kadijk J.A., Cornel J.H., Kamp O., et al. Lenient versus Strict Rate Control in Patients with Atrial Fibrillation. N. Engl. J. Med. 2010;362:1363–1373. doi: 10.1056/NEJMoa1001337. - DOI - PubMed
-
- Netzler P.C. Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation. Yearb. Cardiol. 2012;2012:490–492. doi: 10.1016/j.ycar.2012.02.044. - DOI
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
