

The Spectrum of MRI Findings in Dengue Encephalitis
- PMID: 36237802
- PMCID: PMC9553126
- DOI: 10.7759/cureus.29048
The Spectrum of MRI Findings in Dengue Encephalitis
Abstract
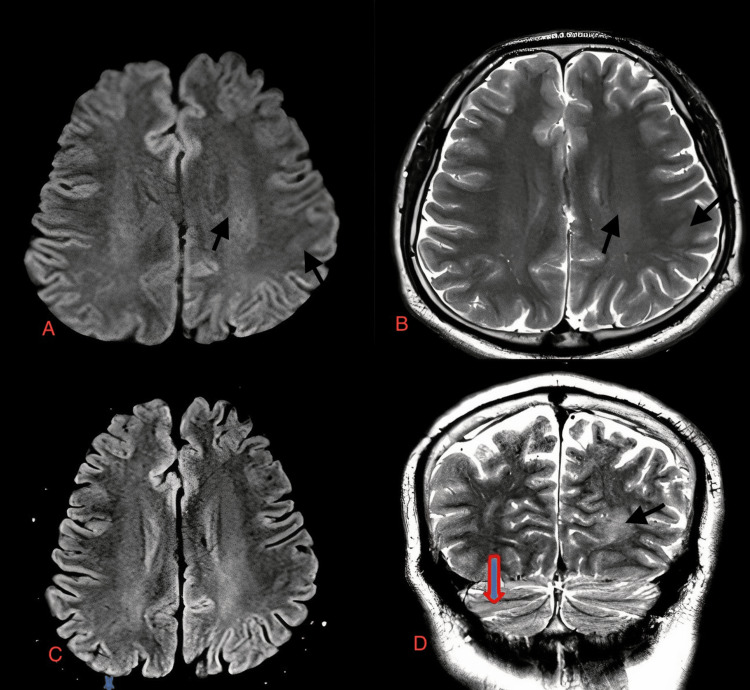
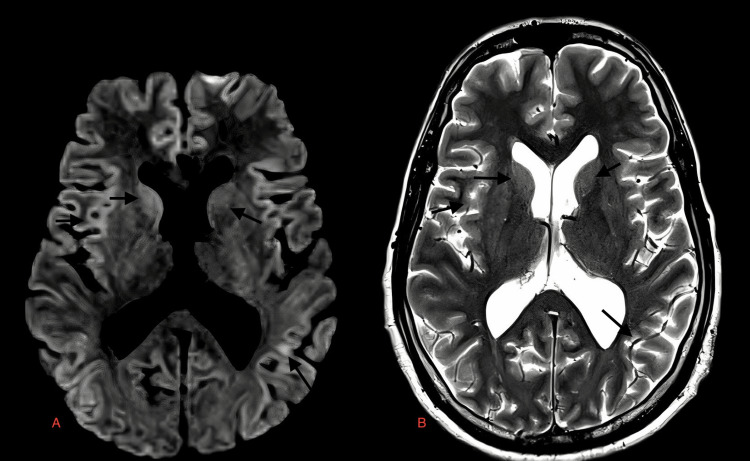
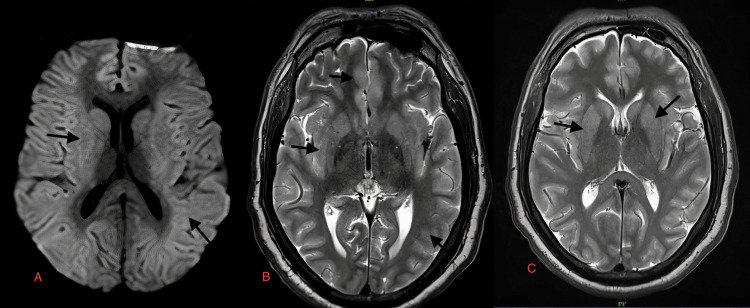
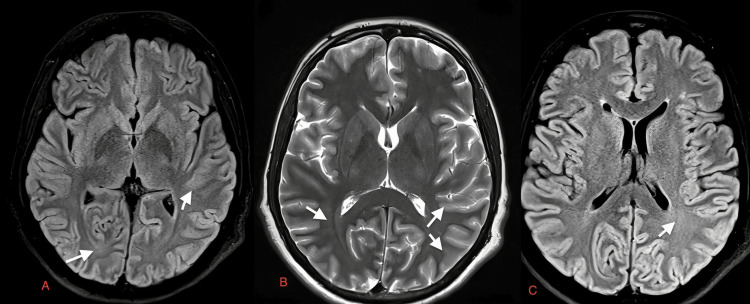
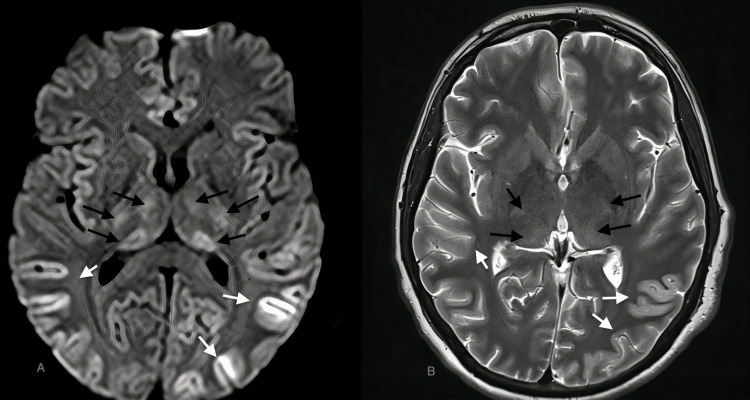
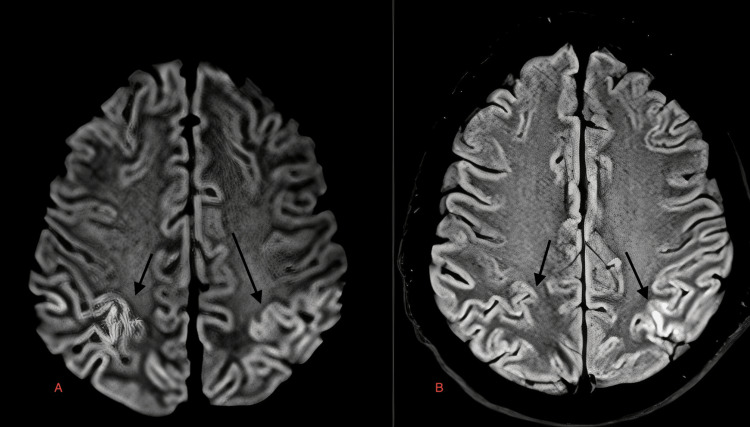
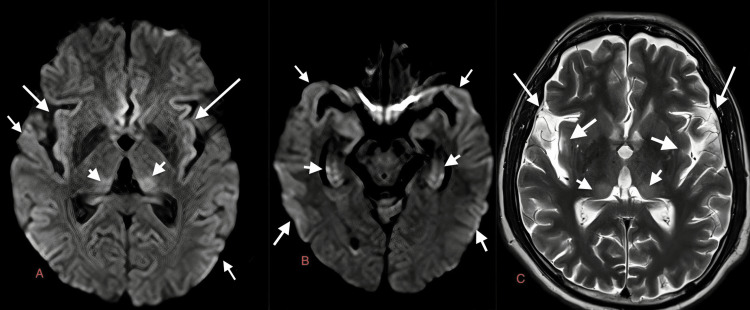
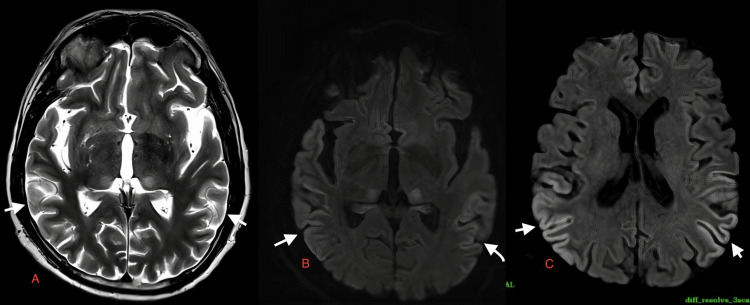
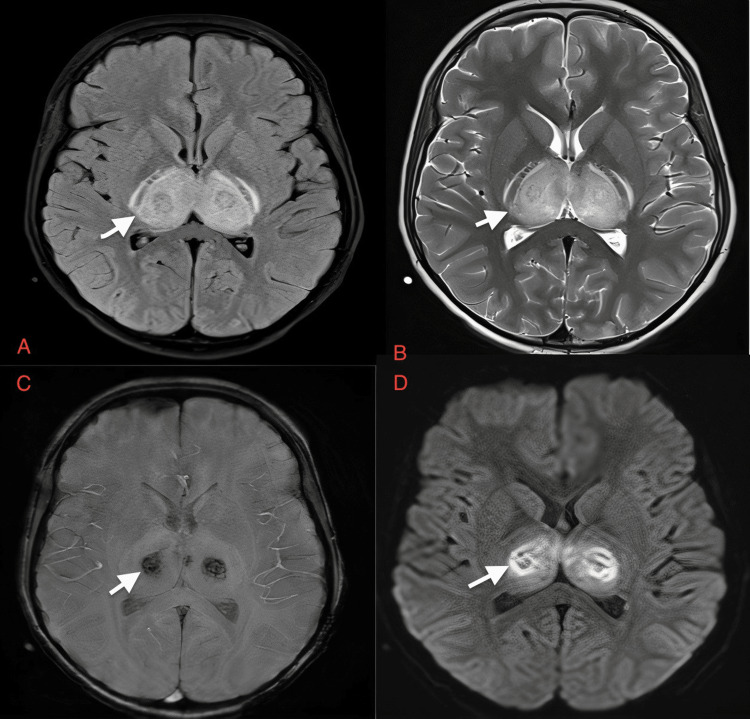
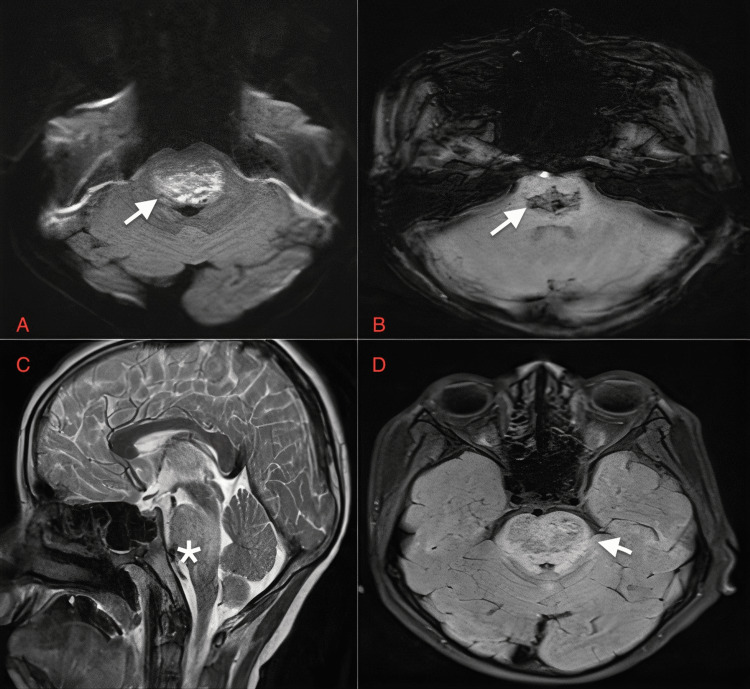
Background In this study, we aimed to describe eight cases of dengue encephalitis along with their magnetic resonance imaging (MRI) findings. Dengue encephalitis is caused by an arbovirus that has four strains DENV1-DENV4. The dengue virus is usually non-neurotropic but DENV2 & DENV3 are neurotropic. Dengue encephalitis is characterized by headaches, seizures, and altered consciousness. Methodology At our facility, we performed 3T MRI on eight suspected cases of dengue encephalitis using the criteria established by Varatharaj et al. We were able to diagnose dengue encephalitis based on the proposed criteria which included symptoms, serology, cerebrospinal fluid (CSF) analysis results, MRI findings, and routine blood laboratory workup in dengue encephalitis. Because numerous brain regions are potentially impacted in severe cases of dengue encephalitis, an MRI of the brain can reveal the severity of the condition. In deteriorating situations, it may detect whether or not further regions are being impacted. Hence, MRI should be done in all suspected cases of dengue encephalitis. Results The changes observed on MRI of the eight cases were in the supra-tentorium (deep periventricular white matter, subcortical white matter, and deep gray matter of the brain, which includes basal ganglia and thalami), infra-tentorium (cerebellar white matter and brainstem, which includes pons), and occasionally in cortical gray matter. The MRI showed mild-to-moderate hyperintensities on T2-weighted images and fluid-attenuated inversion recovery sequence (FLAIR); diffusion restriction is seen on diffusion-weighted images. The neurological clinical features included non-localizing signs and symptoms such as altered mental status, headache with vomiting, and fever. Conclusions The commonly affected areas of the brain in dengue encephalitis are the basal ganglia, thalamus, brainstem, cerebellum, cortical white matter, periventricular white matter, and cortical gray matter, which are all hyperintense on T2-weighted images and FLAIR. The lesions are iso or hypointense on T1-weighted images and micro-hemorrhages appear as blooming on susceptibility-weighted MRI. MRI is a crucial initial investigation in suspected cases of dengue encephalitis and known cases of dengue fever experiencing worsening neurological conditions.
Keywords: 3-tesla mri; dengue fever/complications; expanded dengue syndrome; infectious encephalitis; mri findings.
Copyright © 2022, LNU et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Spectrum of findings on magnetic resonance imaging of the brain in patients with neurological manifestations of dengue fever.Radiol Bras. 2017 Sep-Oct;50(5):285-290. doi: 10.1590/0100-3984.2016.0048. Radiol Bras. 2017. PMID: 29085161 Free PMC article.
-
Leptomeningeal enhancement of myelin oligodendrocyte glycoprotein antibody-associated encephalitis: uncovering novel markers on contrast-enhanced fluid-attenuated inversion recovery images.Front Immunol. 2023 Jun 20;14:1152235. doi: 10.3389/fimmu.2023.1152235. eCollection 2023. Front Immunol. 2023. PMID: 37409120 Free PMC article.
-
Acute hemorrhagic encephalitis: An unusual presentation of dengue viral infection.Indian J Radiol Imaging. 2015 Jan-Mar;25(1):52-5. doi: 10.4103/0971-3026.150145. Indian J Radiol Imaging. 2015. PMID: 25709166 Free PMC article.
-
[Radiological diagnosis of viral encephalitis].Nihon Rinsho. 1997 Apr;55(4):815-21. Nihon Rinsho. 1997. PMID: 9103877 Review. Japanese.
-
Anti-N-methyl-D-aspartate receptor encephalitis concomitant with multifocal subcortical white matter lesions on magnetic resonance imaging: a case report and review of the literature.BMC Neurol. 2015 Jul 8;15:107. doi: 10.1186/s12883-015-0366-5. BMC Neurol. 2015. PMID: 26152327 Free PMC article. Review.
Cited by
-
Rare case of dengue encephalitis with extensive brain lesions from Pakistan.BMJ Case Rep. 2022 Nov 25;15(11):e250271. doi: 10.1136/bcr-2022-250271. BMJ Case Rep. 2022. PMID: 36428031 Free PMC article.
-
Atypical manifestations of Dengue fever: case series in tertiary care hospital in Nepal.BJR Case Rep. 2025 Jul 18;11(4):uaaf038. doi: 10.1093/bjrcr/uaaf038. eCollection 2025 Jul. BJR Case Rep. 2025. PMID: 40800585 Free PMC article. Review.
-
The split apparent diffusion coefficient sign: A novel magnetic resonance imaging biomarker for cortical pathology with possible implications in autoimmune encephalitis.Neuroradiol J. 2024 Apr;37(2):206-213. doi: 10.1177/19714009231224416. Epub 2023 Dec 26. Neuroradiol J. 2024. PMID: 38146643 Free PMC article.
-
Severe dengue encephalitis showcasing the "double doughnut sign" on MRI: A case report.Radiol Case Rep. 2025 Jul 5;20(9):4820-4824. doi: 10.1016/j.radcr.2025.06.043. eCollection 2025 Sep. Radiol Case Rep. 2025. PMID: 40686795 Free PMC article.
-
An Intriguing Case of Expanded Dengue Syndrome With Co-existing Encephalitis, Pancreatitis, and Hepatitis: The Classic Thalamic "Double-Doughnut" Sign Revisited.Neurohospitalist. 2024 Jul;14(3):316-321. doi: 10.1177/19418744241230730. Epub 2024 Jan 28. Neurohospitalist. 2024. PMID: 38894998 Free PMC article.
References
-
- Schaefer TJ, Panda PK, Wolford RW. Treasure Island, FL: StatPearls Publishing; 2022. Dengue Fever. - PubMed
-
- The involvement of neuroinflammation in dengue viral disease: importance of innate and adaptive immunity. Niranjan R, Muthukumaravel S, Jambulingam P. Neuroimmunomodulation. 2019;26:111–118. - PubMed
-
- Neurological manifestations of dengue infection. Solomon T, Dung NM, Vaughn DW, et al. Lancet. 2000;355:1053–1059. - PubMed
-
- Encephalitis in the clinical spectrum of dengue infection. Varatharaj A. Neurol India. 2010;58:585–591. - PubMed
LinkOut - more resources
Full Text Sources