

Upper thoracic empyema and concomitant superior vena cava syndrome treated with reconstructive surgery using a pedicled omental flap
- PMID: 36237890
- PMCID: PMC9529635
- DOI: 10.18999/nagjms.84.3.648
Upper thoracic empyema and concomitant superior vena cava syndrome treated with reconstructive surgery using a pedicled omental flap
Abstract
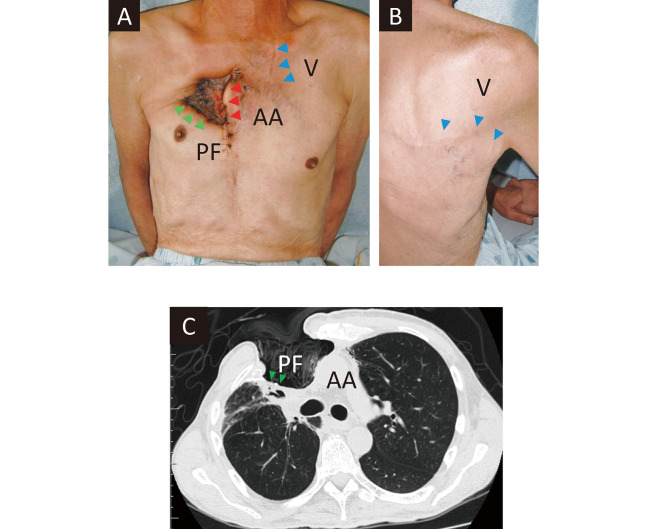
Superior vena cava (SVC) syndrome refers to a constellation of symptoms secondary to obstruction of blood flow through the SVC. In this condition, venous blood that usually drains into the SVC is diverted into the inferior vena cava (IVC) via collateral veins. Reconstructive surgery is challenging in such cases owing to the anomalous venous system. In this case report, we describe reconstructive surgery using a pedicled omental flap in a patient with upper thoracic empyema and concomitant SVC syndrome. A 68-year-old man underwent resection of malignant thymoma, the bilateral brachiocephalic veins, and a part of the right upper lobe, followed by polytetrafluoroethylene (PTFE) graft placement for venous system reconstruction, 2 years prior to presentation. He developed postoperative upper thoracic cavity empyema, which necessitated PTFE graft removal. Although the infection was controlled after 2 months, multiple right upper lobe pulmonary fistulas persisted, and the patient was referred to our department for further evaluation. Contrast-enhanced computed tomography revealed SVC syndrome characterized by SVC obstruction and consequent drainage of venous blood from the upper trunk into the IVC via collateral vessels. We debrided necrotic and infected tissues, and a pedicled omental flap was placed for upper lobe fistula coverage. The patient showed an uncomplicated postoperative course, and no recurrent empyema or pulmonary fistulas were observed 3 years postoperatively. Flaps associated with the SVC system show high venous pressures. The use of a pedicled omental flap was deemed feasible because this graft reaches the upper thorax even though it is associated with the IVC system.
Keywords: empyema; omental flap; reconstructive surgery; superior vena cava syndrome.
Conflict of interest statement
No funding was received for this study, and all authors declare that they have no conflict of interest.
Figures



Similar articles
-
Thrombectomy and SVC reconstruction due to infective thrombus.J Cardiovasc Surg (Torino). 2002 Feb;43(1):91-3. J Cardiovasc Surg (Torino). 2002. PMID: 11803337
-
Long Term Results of Bypass Graft to the Right Atrium in the Management of Superior Vena Cava Syndrome in Dialysis Patients.Ann Vasc Surg. 2021 Jul;74:321-329. doi: 10.1016/j.avsg.2021.01.099. Epub 2021 Mar 6. Ann Vasc Surg. 2021. PMID: 33689760
-
Where there is blood, there is a way: unusual collateral vessels in superior and inferior vena cava obstruction.Radiographics. 2010 Jan;30(1):67-78. doi: 10.1148/rg.301095724. Radiographics. 2010. PMID: 20083586
-
Unique Medley of Cardinal Veins: Duplicated Superior and Inferior Venae Cavae With Left Renal Agenesis and Hemiazygos Continuation of Left Inferior Vena Cava With Drainage Into Left Atrium.Vasc Endovascular Surg. 2022 Apr;56(3):330-334. doi: 10.1177/15385744211051493. Epub 2022 Feb 7. Vasc Endovascular Surg. 2022. PMID: 35125023 Review.
-
INTRAVASCULAR LIPOMA OF THE RIGHT BRACHIOCEPHALIC VEIN AND SUPERIOR VENA CAVA: A CASE REPORT AND LITERATURE REVIEW.Georgian Med News. 2021 Feb;(311):33-36. Georgian Med News. 2021. PMID: 33814386 Review.
References
-
- Kato H, Yasue Y, Kohyama K. Is a unilateral reconstructed internal jugular vein suitable as the recipient vein in free flap surgery after bilateral internal jugular vein resection? [in Japanese]. J Jpn Soc Reconstr Microsurg. 2018;31(2):93–97.doi:10.11270/jjsrm.31.93. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical