

Edema formation in congestive heart failure and the underlying mechanisms
- PMID: 36237903
- PMCID: PMC9553007
- DOI: 10.3389/fcvm.2022.933215
Edema formation in congestive heart failure and the underlying mechanisms
Abstract
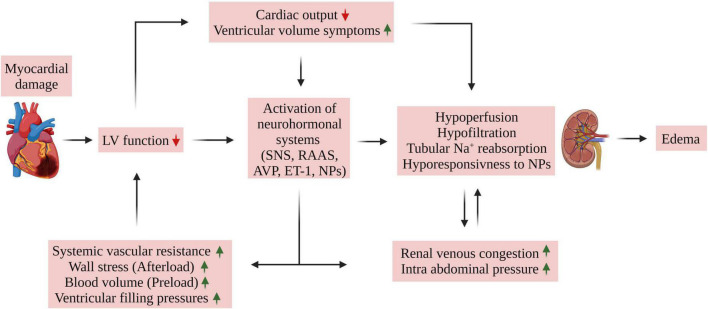
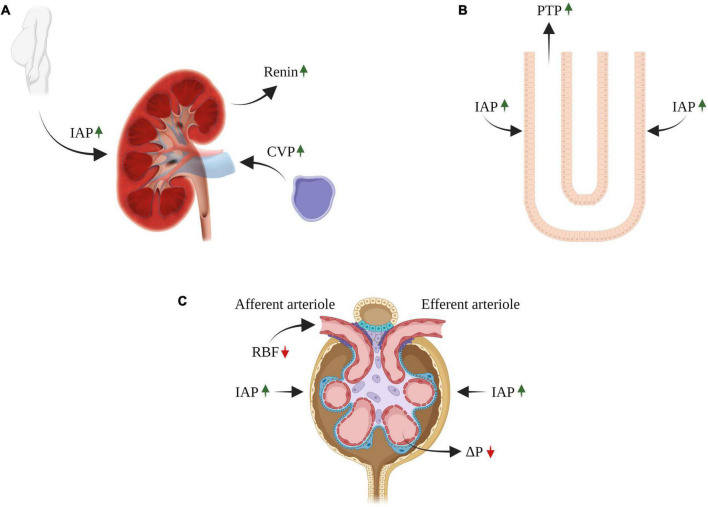
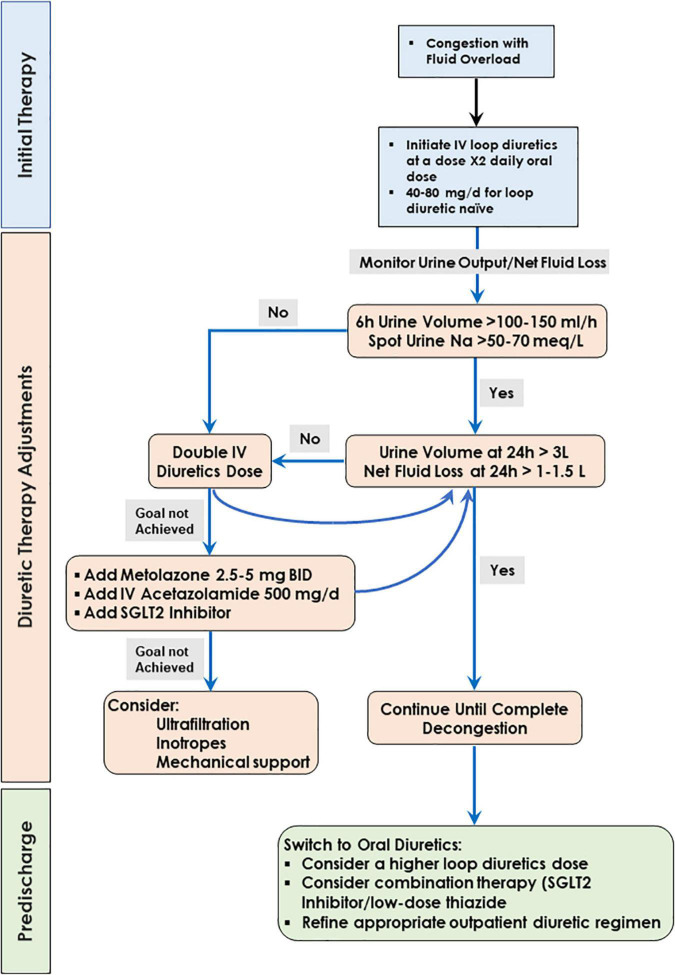
Congestive heart failure (HF) is a complex disease state characterized by impaired ventricular function and insufficient peripheral blood supply. The resultant reduced blood flow characterizing HF promotes activation of neurohormonal systems which leads to fluid retention, often exhibited as pulmonary congestion, peripheral edema, dyspnea, and fatigue. Despite intensive research, the exact mechanisms underlying edema formation in HF are poorly characterized. However, the unique relationship between the heart and the kidneys plays a central role in this phenomenon. Specifically, the interplay between the heart and the kidneys in HF involves multiple interdependent mechanisms, including hemodynamic alterations resulting in insufficient peripheral and renal perfusion which can lead to renal tubule hypoxia. Furthermore, HF is characterized by activation of neurohormonal factors including renin-angiotensin-aldosterone system (RAAS), sympathetic nervous system (SNS), endothelin-1 (ET-1), and anti-diuretic hormone (ADH) due to reduced cardiac output (CO) and renal perfusion. Persistent activation of these systems results in deleterious effects on both the kidneys and the heart, including sodium and water retention, vasoconstriction, increased central venous pressure (CVP), which is associated with renal venous hypertension/congestion along with increased intra-abdominal pressure (IAP). The latter was shown to reduce renal blood flow (RBF), leading to a decline in the glomerular filtration rate (GFR). Besides the activation of the above-mentioned vasoconstrictor/anti-natriuretic neurohormonal systems, HF is associated with exceptionally elevated levels of atrial natriuretic peptide (ANP) and brain natriuretic peptide (BNP). However, the supremacy of the deleterious neurohormonal systems over the beneficial natriuretic peptides (NP) in HF is evident by persistent sodium and water retention and cardiac remodeling. Many mechanisms have been suggested to explain this phenomenon which seems to be multifactorial and play a major role in the development of renal hyporesponsiveness to NPs and cardiac remodeling. This review focuses on the mechanisms underlying the development of edema in HF with reduced ejection fraction and refers to the therapeutic maneuvers applied today to overcome abnormal salt/water balance characterizing HF.
Keywords: Na+ retention; cardiorenal syndrome; edema; heart failure; intra-abdominal pressure; mechanisms; neurohumoral; renal venous congestion.
Copyright © 2022 Abassi, Khoury, Karram and Aronson.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Skorecki K, Winaver J, Abassi Z. Brenner and Rector’s The Kidney. 8th ed. In: Brenner B, Rector F. editors. Amsterdam: Elsevier; (2008). p. 398–458.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous