

Normalisation of High Bone Remodelling due to Oestrogen Deficiency by Traditional Chinese Formulation Kang Shuai Lao Pian in Ovariectomised Rats
- PMID: 36237992
- PMCID: PMC9553853
- DOI: 10.7150/ijms.75915
Normalisation of High Bone Remodelling due to Oestrogen Deficiency by Traditional Chinese Formulation Kang Shuai Lao Pian in Ovariectomised Rats
Abstract
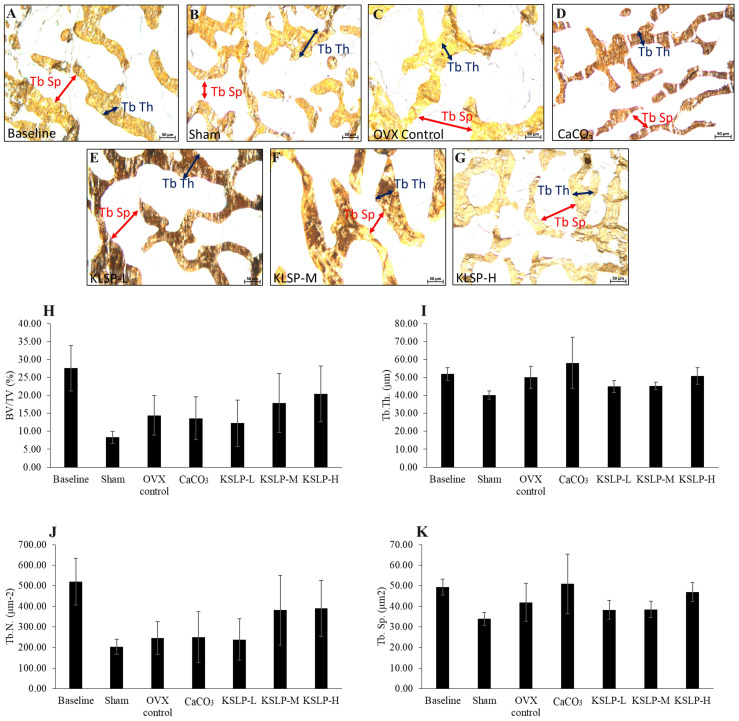
Postmenopausal osteoporosis transpires due to excessive osteoclastic bone resorption and insufficient osteoblastic bone formation in the presence of oestrogen insufficiency. Kang Shuai Lao Pian (KSLP) is a red ginseng-based traditional Chinese medicine known for its anti-ageing properties. However, studies on its effect on bone loss are lacking. Thus, the current study examined the skeletal protective effects of KSLP in an ovariectomised rodent bone loss model. Three-month-old female Sprague Dawley rats (n=42) were randomised into baseline, sham and ovariectomised (OVX) groups. The OVX rats were supplemented with low- (KSLP-L; 0.15 g/kg), medium- (KSLP-M; 0.30 g/kg), high-dose KSLP (KSLP-H; 0.45 g/kg) or calcium carbonate (1% w/v). The daily supplementation of KSLP was performed via oral gavage for eight weeks. Gavage stress was stimulated in the ovariectomised control with distilled water. The rats were euthanised at the end of the study. Whole-body and femoral bone mineral content and density scans were performed at baseline and every four weeks. Blood samples were obtained for the determination of bone remodelling markers. Histomorphometry and biomechanical strength testing were performed on femurs and tibias. High bone remodelling typically due to oestrogen deficiency, indicated by the elevated bone formation and resorption markers, osteoclast surface, single-labelled surface and mineralising surface/bone surface ratio, was observed in the untreated OVX rats. Whole-body BMD adjusted to body weight and Young's modulus decreased significantly in the untreated OVX rats. High-dose KSLP supplementation counteracted these degenerative changes. In conclusion, KSLP improves bone health by normalising bone remodelling, thereby preventing bone loss and decreased bone strength caused by oestrogen deficiency. Its anti-osteoporosis effects should be validated in patients with postmenopausal osteoporosis.
Keywords: Traditional Chinese medicine; postmenopausal osteoporosis; skeletal health.
© The author(s).
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures





Similar articles
-
Suppression of high bone remodelling by E'Jiao in ovariectomised rats.Biomed Pharmacother. 2022 Aug;152:113265. doi: 10.1016/j.biopha.2022.113265. Epub 2022 Jun 13. Biomed Pharmacother. 2022. PMID: 35709654
-
Self-emulsified annatto tocotrienol improves bone histomorphometric parameters in a rat model of oestrogen deficiency through suppression of skeletal sclerostin level and RANKL/OPG ratio.Int J Med Sci. 2021 Sep 9;18(16):3665-3673. doi: 10.7150/ijms.64045. eCollection 2021. Int J Med Sci. 2021. PMID: 34790038 Free PMC article.
-
The effects of E'Jiao on body composition, bone marrow adiposity and skeletal redox status in ovariectomised rats.Int J Med Sci. 2023 Oct 9;20(13):1711-1721. doi: 10.7150/ijms.84604. eCollection 2023. Int J Med Sci. 2023. PMID: 37928881 Free PMC article.
-
Traditional Chinese Medicine Formula Kang Shuai Lao Pian Improves Obesity, Gut Dysbiosis, and Fecal Metabolic Disorders in High-Fat Diet-Fed Mice.Front Pharmacol. 2020 Mar 25;11:297. doi: 10.3389/fphar.2020.00297. eCollection 2020. Front Pharmacol. 2020. PMID: 32269525 Free PMC article.
-
A traditional Chinese herbal preparation, Er-Zhi-Wan, prevent ovariectomy-induced osteoporosis in rats.J Ethnopharmacol. 2011 Nov 18;138(2):279-85. doi: 10.1016/j.jep.2011.09.030. Epub 2011 Oct 5. J Ethnopharmacol. 2011. PMID: 22001072 Review.
Cited by
-
Study on the association of the microstructure and bone metabolism in the osteoporotic femoral head.Mol Biol Rep. 2023 Sep;50(9):7437-7444. doi: 10.1007/s11033-023-08505-2. Epub 2023 Jul 21. Mol Biol Rep. 2023. PMID: 37479877 Free PMC article.
-
Evaluation of bone-protecting effects of palm carotene mixture in two- and three-dimensional osteoblast/osteoclast co-culture systems.Int J Med Sci. 2025 Jan 6;22(3):585-603. doi: 10.7150/ijms.103445. eCollection 2025. Int J Med Sci. 2025. PMID: 39898246 Free PMC article.
References
-
- Eastell R, O'Neill TW, Hofbauer LC, Langdahl B, Reid IR, Gold DT. et al. Postmenopausal osteoporosis. Nat Rev Dis Primers. 2016;2:16069. - PubMed
-
- Lorentzon M, Johansson H, Harvey NC, Liu E, Vandenput L, McCloskey EV. et al. Osteoporosis and fractures in women: the burden of disease. Climacteric. 2022;25:4–10. - PubMed
-
- Black DM, Rosen CJ. Clinical Practice. Postmenopausal Osteoporosis. N Engl J Med. 2016;374:254–62. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
