

[Immunoglobulin G4-Related Disease in the Thorax: Imaging Findings and Differential Diagnosis]
- PMID: 36238052
- PMCID: PMC9514412
- DOI: 10.3348/jksr.2021.0078
[Immunoglobulin G4-Related Disease in the Thorax: Imaging Findings and Differential Diagnosis]
Abstract
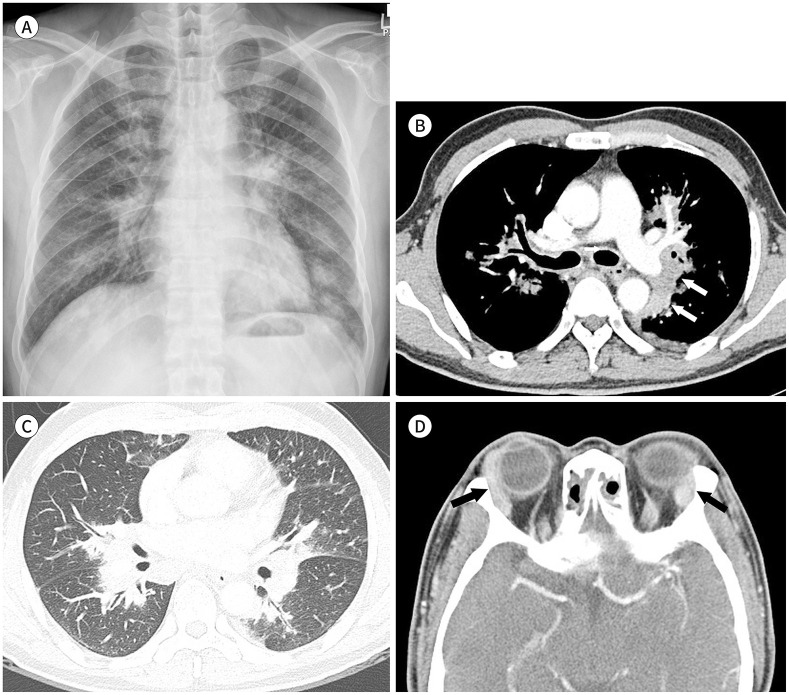
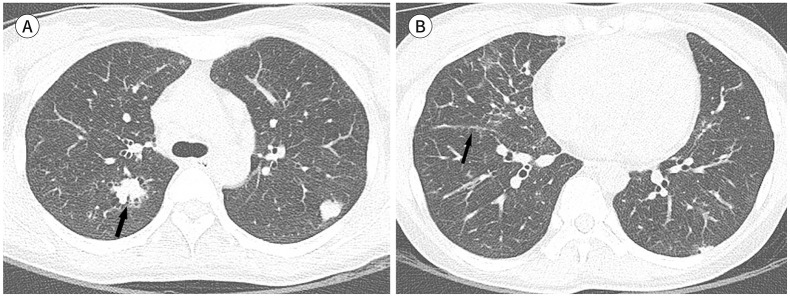
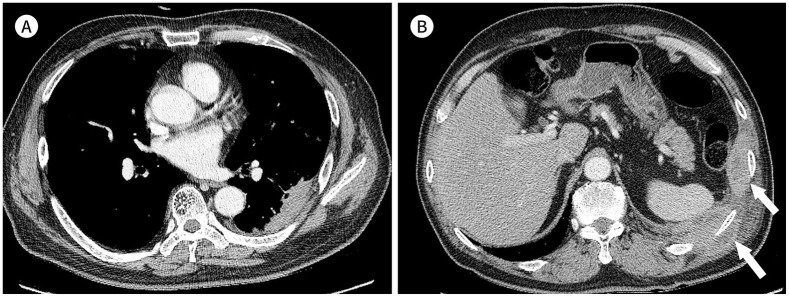
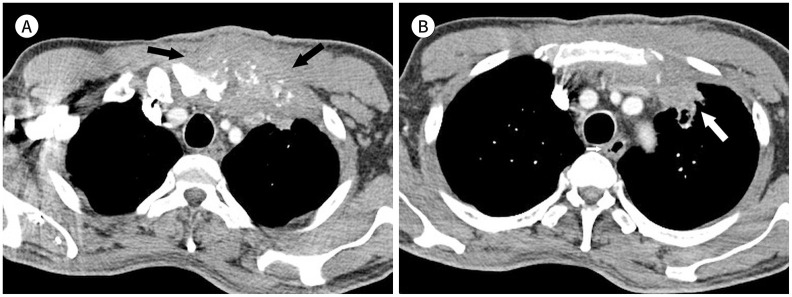
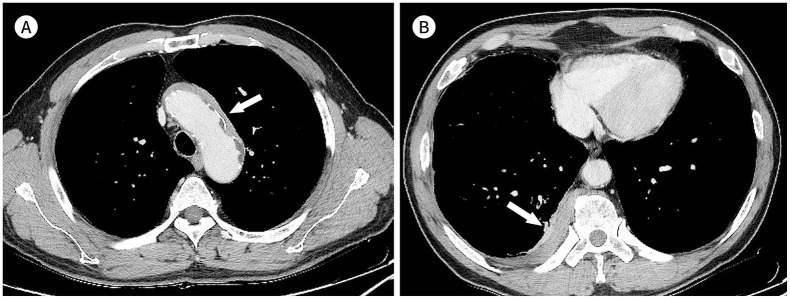
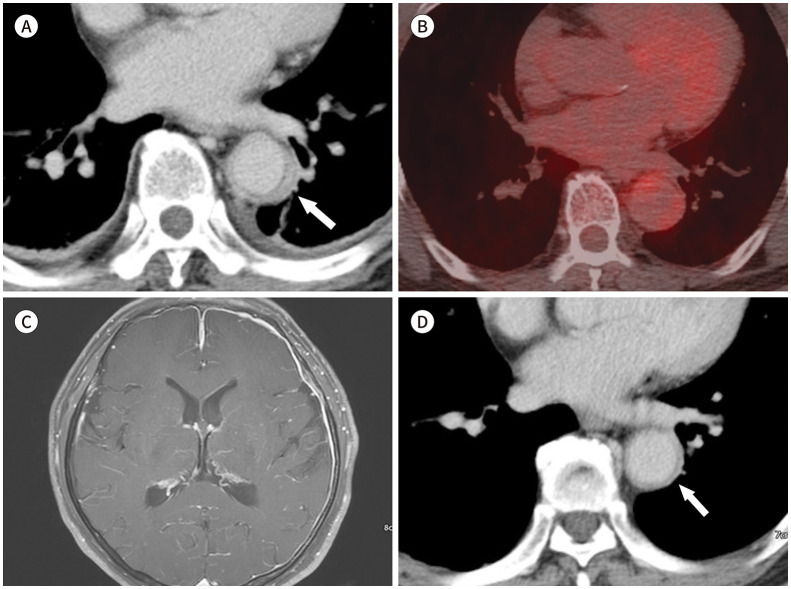
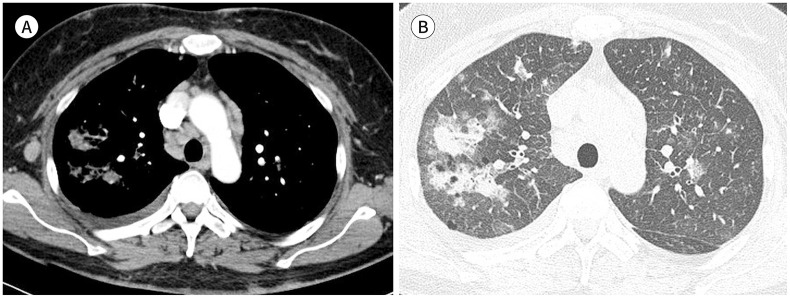
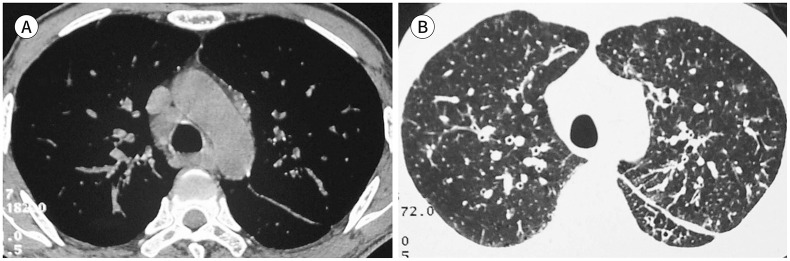
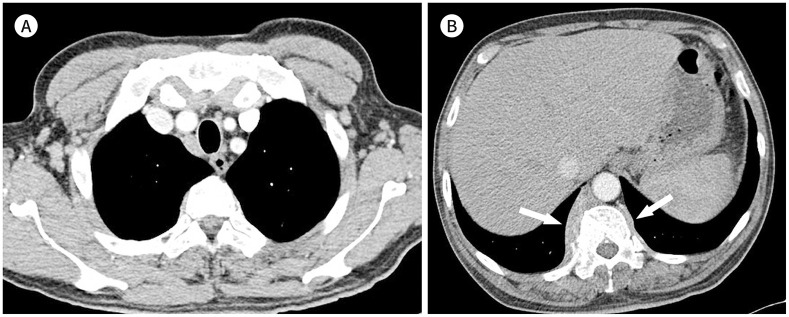
Immunoglobulin G4-related disease (IgG4-RD) is a chronic inflammatory condition involving multiple organs, including the salivary or lacrimal glands, orbit, pancreas, bile duct, liver, kidney, retroperitoneum, aorta, lung, and lymph nodes. It is histologically characterized by tissue infiltration with lymphocytes and IgG4-secreting plasma cells, storiform fibrosis, and obliterative phlebitis. In the thoracic involvement of IgG4-RD, mediastinal lymphadenopathy and perilymphangitic interstitial thickening of the lung are the most common findings. Peribronchovascular and septal thickening and paravertebral band-like soft tissue are characteristic findings of IgG4-RD. Other findings include pulmonary nodules or masses, ground-glass opacity, alveolar interstitial thickening, pleural effusion or thickening, mass in the chest wall or mediastinum, and arteritis involving the aorta and coronary artery. Radiologic differential diagnosis of various malignancies, infections, and inflammatory conditions is needed. In this review, we describe the imaging findings of IgG4-RD and the radiologic differential diagnoses in the thorax.
면역글로불린G4 연관 질환(immunoglobulin G4-related disease; 이하 IgG4-RD)는 IgG4를 생산하는 면역세포에 의한 만성 염증성질환으로, 주로 타액선, 누액선, 안와, 췌장, 담도, 간, 신장, 후복막, 대동맥, 폐, 림프절 등 다양한 장기를 침범하고, 조직학적으로 IgG4 양성 형질세포와 림프구의 침윤 및 나선형의 섬유화(storiform fibrosis), 폐색정맥염(obliterative phlebitis)을 특징으로 한다. IgG4-RD의 흉부 침범에서 가장 흔한 소견은 종격동 림프절 비대와 폐의 림프관주위 간질 비후이다. 폐의 기관지혈관주위 간질 비후와 우측 척추곁 밴드형 연부조직은 IgG4-RD의 특징적 소견이고, 그 외에도 폐결절 혹은 종괴, 간유리음영, 폐포 간질비후, 흉막삼출 및 비후, 흉벽이나 종격동 종괴, 대동맥과 관상동맥의 혈관염이 발생할 수 있다. 영상의학적으로는 악성 종양이나 감염 및 다양한 염증성질환과의 감별진단이 필요하다. 본 연구에서는 흉부에서 발생하는 IgG4-RD의 영상 소견과 감별진단에 대해 기술하였다.
Copyrights © 2021 The Korean Society of Radiology.
Conflict of interest statement
Conflicts of Interest: The authors have no potential conflicts of interest to disclose.
Figures



Similar articles
-
Immunoglobulin G4-related hepatobiliary disease.Semin Diagn Pathol. 2019 Nov;36(6):423-433. doi: 10.1053/j.semdp.2019.07.007. Epub 2019 Jul 24. Semin Diagn Pathol. 2019. PMID: 31358425 Review.
-
Intrathoracic Involvements of Immunoglobulin G4-Related Sclerosing Disease.Medicine (Baltimore). 2015 Dec;94(50):e2150. doi: 10.1097/MD.0000000000002150. Medicine (Baltimore). 2015. PMID: 26683924 Free PMC article.
-
Immunoglobulin G4-Related Disease: What an Allergist Should Know.J Investig Allergol Clin Immunol. 2021 Jun 22;31(3):212-227. doi: 10.18176/jiaci.0633. Epub 2020 Jul 30. J Investig Allergol Clin Immunol. 2021. PMID: 32732179 Review.
-
Thoracic manifestations of IgG4-related disease.Respirology. 2023 Feb;28(2):120-131. doi: 10.1111/resp.14422. Epub 2022 Nov 27. Respirology. 2023. PMID: 36437514 Free PMC article. Review.
-
Thoracic involvement and imaging patterns in IgG4-related disease.Eur Respir Rev. 2021 Oct 5;30(162):210078. doi: 10.1183/16000617.0078-2021. Print 2021 Dec 31. Eur Respir Rev. 2021. PMID: 34615698 Free PMC article. Review.
Cited by
-
Immunoglobulin G4-Related Lung Disease Mimicking Lung Cancer: Two Case Reports.J Korean Soc Radiol. 2022 Sep;83(5):1168-1174. doi: 10.3348/jksr.2021.0158. Epub 2022 May 23. J Korean Soc Radiol. 2022. PMID: 36276215 Free PMC article.
References
-
- Kamisawa T, Zen Y, Pillai S, Stone JH. IgG4-related disease. Lancet. 2015;385:1460–1471. - PubMed
-
- Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med. 2012;366:539–551. - PubMed
-
- Corcoran JP, Culver EL, Anstey RM, Talwar A, Manganis CD, Cargill TN, et al. Thoracic involvement in IgG4-related disease in a UK-based patient cohort. Respir Med. 2017;132:117–121. - PubMed
-
- Zhang Z, Guan W, Lin Q, Yu W. Thoracic paravertebral involvement in patients with IgG4-related disease: CT and MR imaging findings. Rheumatology (Oxford) 2020;59:3878–3885. - PubMed
-
- Kanno A, Nishimori I, Masamune A, Kikuta K, Hirota M, Kuriyama S, et al. Nationwide epidemiological survey of autoimmune pancreatitis in Japan. Pancreas. 2012;41:835–839. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
