

Case report: Epidural blood patches are effective in treating intracranial hypotension due to a subarachnoid-pleural fistula
- PMID: 36238858
- PMCID: PMC9551272
- DOI: 10.3389/fsurg.2022.936949
Case report: Epidural blood patches are effective in treating intracranial hypotension due to a subarachnoid-pleural fistula
Abstract
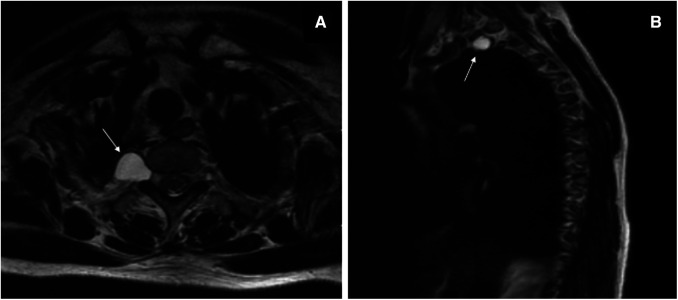
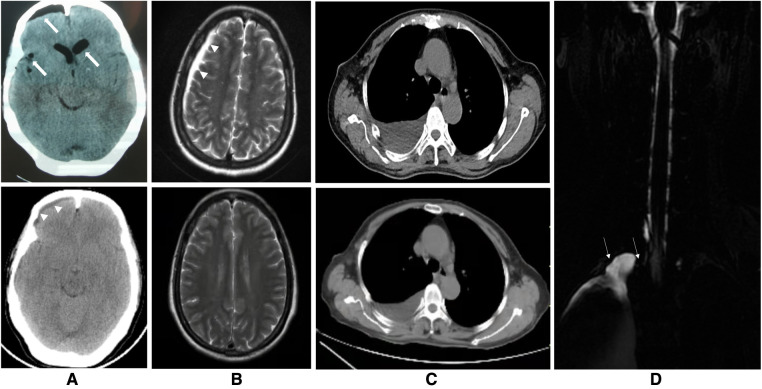
Background: Intracranial hypotension (IH) is usually associated with cerebrospinal fluid (CSF) leakage and/or CSF hypotension, and epidural blood patch (EBP) therapy has been proven to be effective for treating spontaneous IH and post-dural puncture headaches. Tarlov cysts (TCs) are common lesions of the sacral spine. They have rarely been reported in thoracic locations and are even less common in the posterior mediastinum, which can lead to their misdiagnosis as neurogenic tumors.
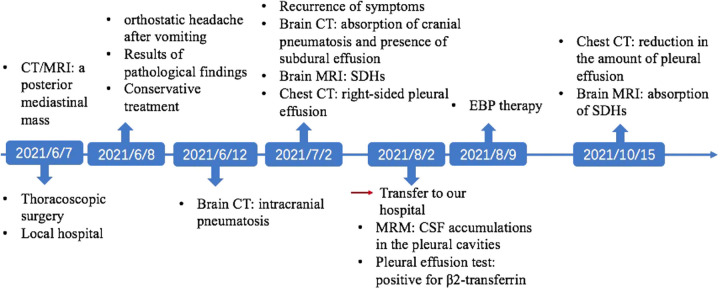
Case presentation: Here, we report the case of a 60-year-old woman who developed an orthostatic headache after the thoracoscopic resection of a TC in the posterior mediastinum that was presumed to be a schwannoma preoperatively. The patient was finally diagnosed with IH caused by a subarachnoid-pleural fistula (SPF) and was cured by targeted EBP treatment.
Conclusion: This is a case to show that a single targeted EBP treatment is effective for a patient with IH caused by an SPF after thoracoscopic resection of a TC. This case reminds us to be vigilant that a TC may be masquerading as a posterior mediastinal neurogenic tumor, and a detailed examination should be performed to identify it before deciding on a surgical procedure. In addition, postural headache after thoracoscopic spinal surgery should be alert to the possibility of IH induced by an SPF. Once it occurs, early treatment is necessary, and targeted EBP treatment can serve as a safe and effective alternative when conservative treatment fails.
Keywords: Tarlov cyst; epidural blood batch; intracranial hypotension; posterior mediastinal mass; subarachnoid-pleural fistula.
© 2022 Huang, Wei, Niu, Yu and He.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources