

Long-term changes in coronary physiology after aortic valve replacement
- PMID: 36239118
- PMCID: PMC9940233
- DOI: 10.4244/EIJ-D-22-00621
Long-term changes in coronary physiology after aortic valve replacement
Abstract
Background: The detrimental effects of long-standing severe aortic stenosis (AS) often include left ventricular hypertrophy (LVH) and exhaustion of coronary flow reserve (CFR), the reversibility of which is unclear after valve replacement.
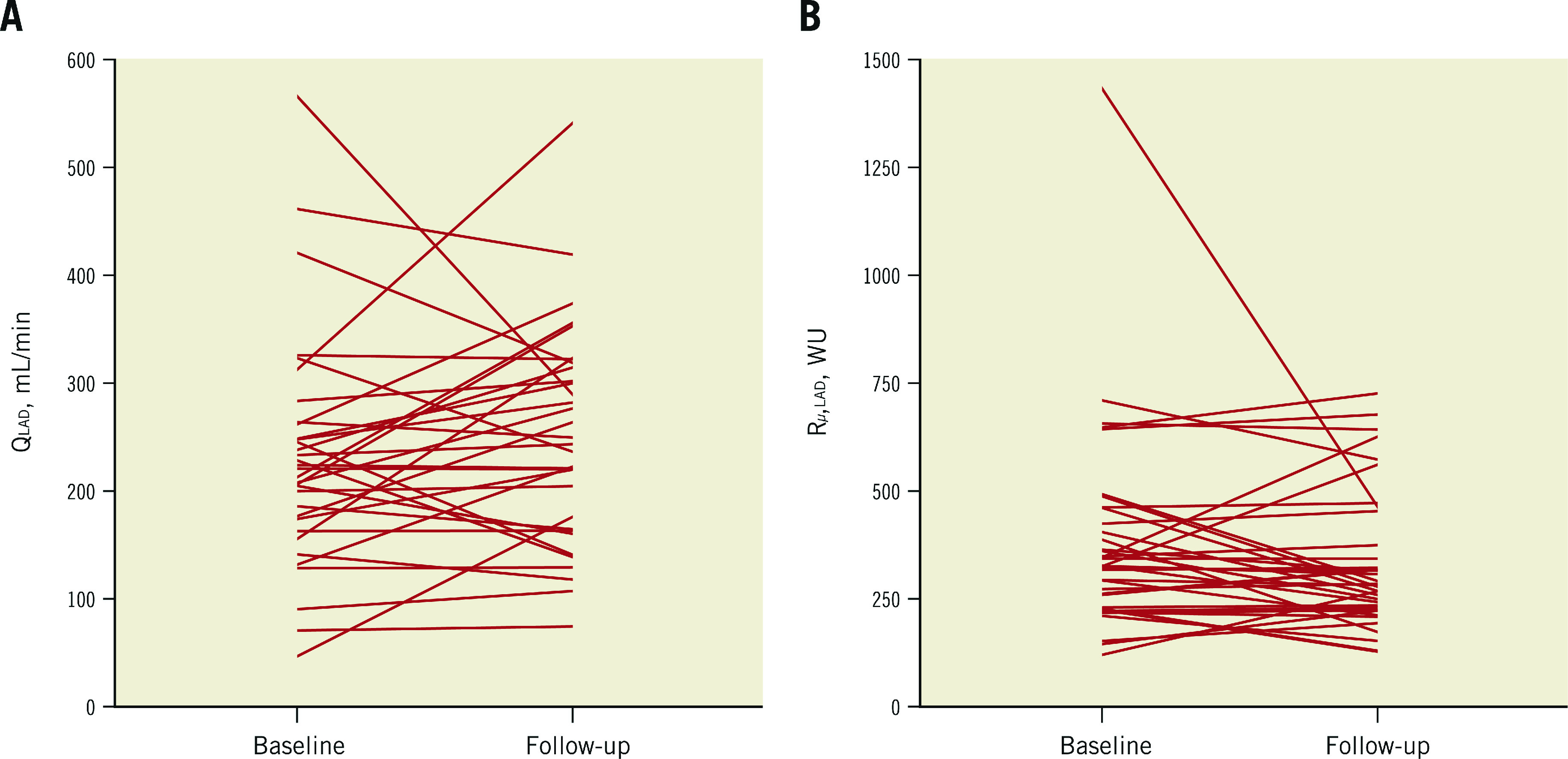
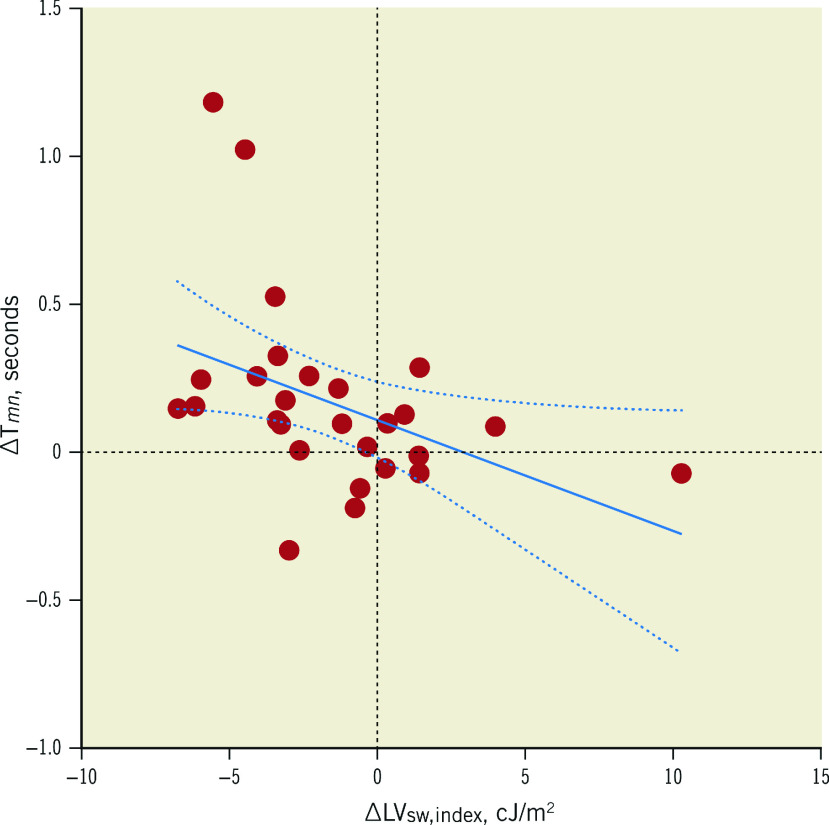
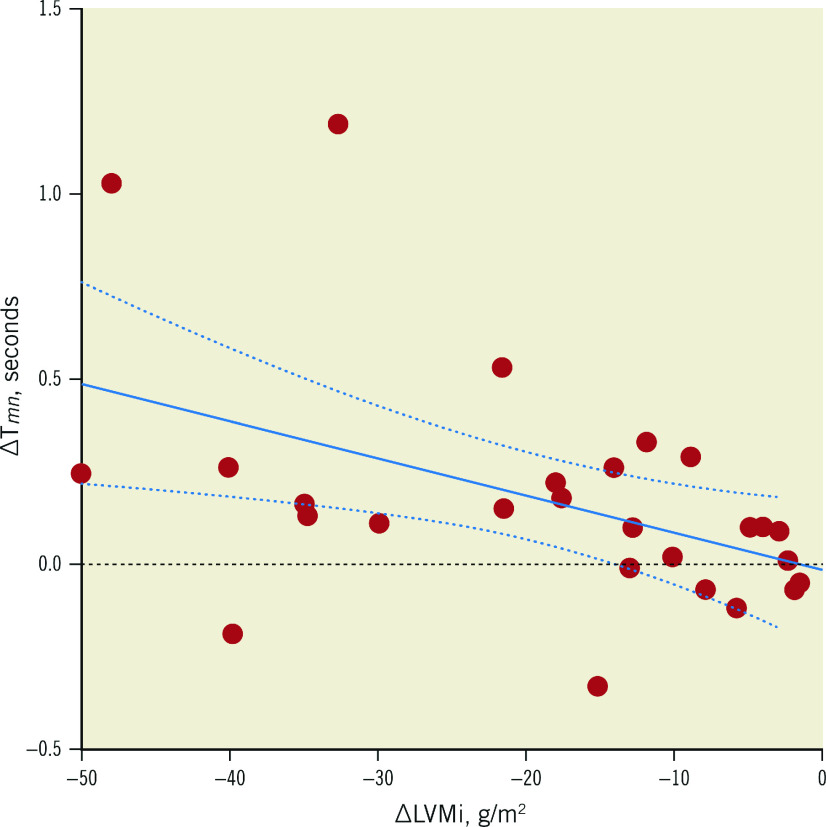
Aims: Our aims were to 1) investigate whether CFR in the left anterior descending artery (LAD) would improve following valve replacement, and if the change was related to changes in hyperaemic coronary flow (QLAD) and minimal microvascular resistance (Rμ,LAD); and 2) investigate the relationship between changes in CFR and changes in left ventricular mass (LVM) and stroke work (LVSW).
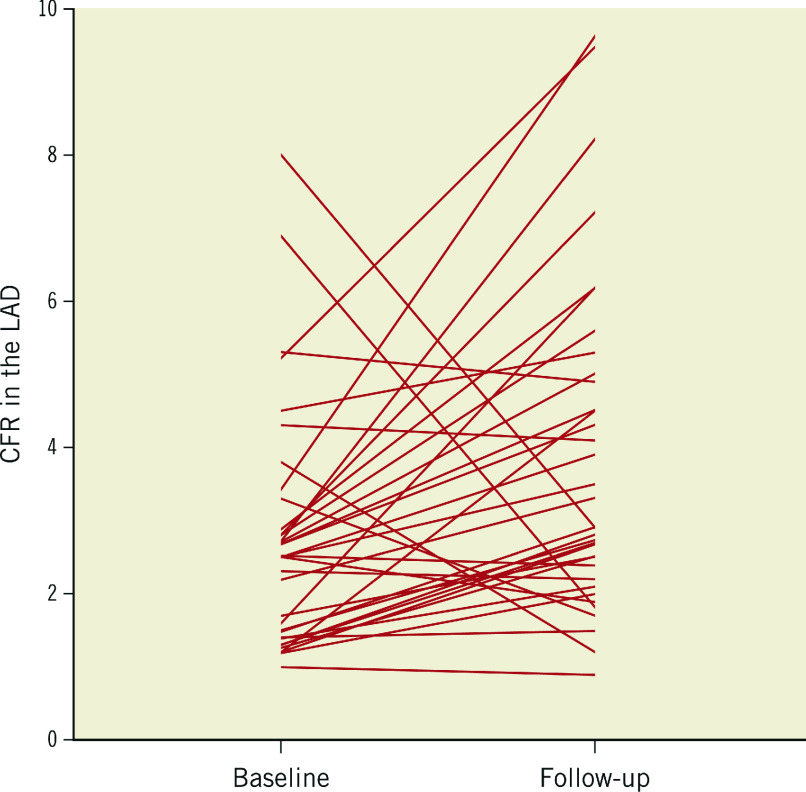
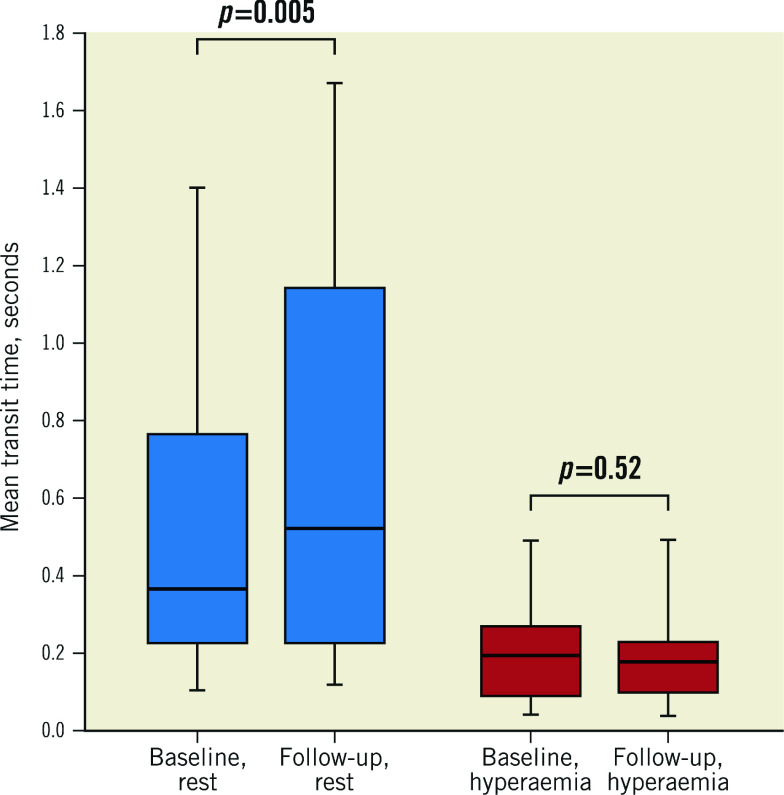
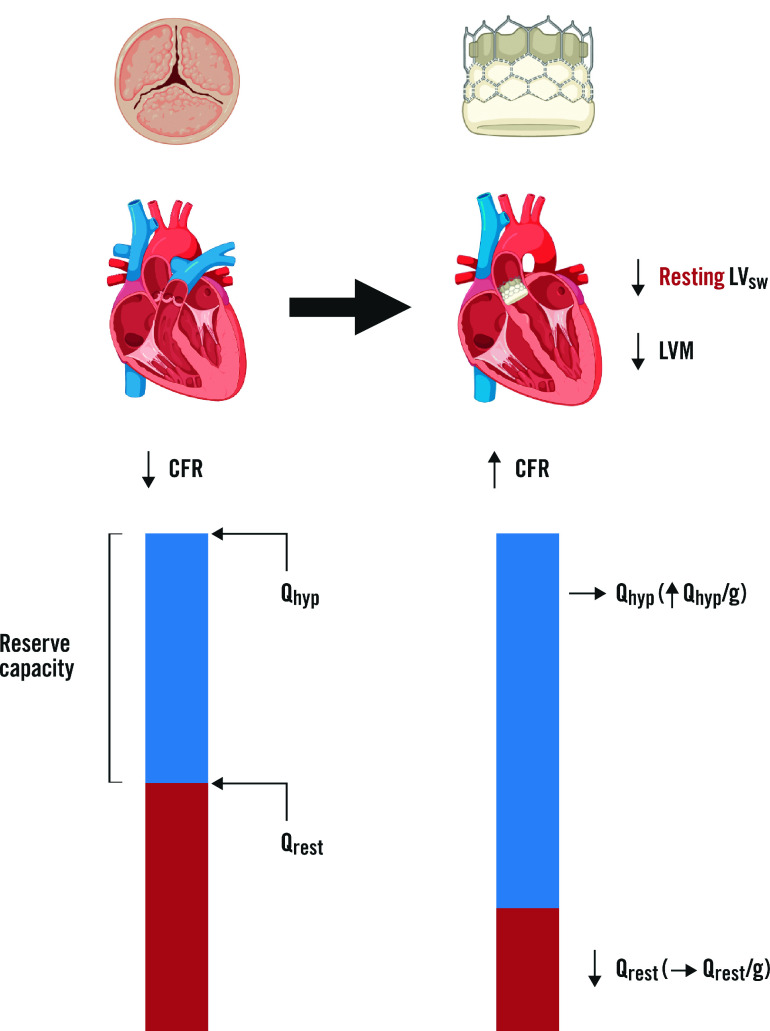
Methods: We measured intracoronary bolus thermodilution-derived CFR, and continuous thermodilution-derived QLAD and Rμ,LAD before and 6 months after aortic valve replacement. Cardiac magnetic resonance imaging was used to quantify left ventricular anatomy and function for the calculation of LVM and LVSW. Results: Thirty-four patients were included (17 patients had transcatheter aortic valve implantation; 14 had surgical valve replacement with a bioprosthesis and 3 with a mechanical prosthesis) who underwent invasive assessment in the LAD. CFR increased from 2.5 (interquartile range [IQR] 1.5-3.3) at baseline to 3.1 (IQR 2.2-5.1) at follow-up (p=0.005), despite no significant change in QLAD (230±106 mL/min to 250±101 mL/min; p=0.26) or Rμ,LAD (347 [IQR 247-463] to 287 [IQR 230-456]; p=0.20). When indexed for LVM, QLAD was 39% (IQR 8-98%) higher at follow-up compared with baseline (p<0.001). The improvement in CFR was correlated with ΔLVSW, r= -0.39; p=0.047. Conclusions: CFR in the LAD increased significantly at follow-up although global hyperaemic flow and minimal microvascular resistance remained unchanged. Thus, a decrease in resting flow was the cause of CFR improvement. CFR improvement was associated with reduction in LVSW.
Conflict of interest statement
K. Arslani has received a research grant from the Swiss Academy of Medical Sciences and the Bangerter Foundation (YTCR 09/19) and the Swiss National Science Foundation (P500PM_202963) outside of the submitted work. The other authors have no conflicts of interest to declare.
Figures
References
-
- Cioffi G, Faggiano P, Vizzardi E, Tarantini L, Cramariuc D, Gerdts E, de Simone. Prognostic effect of inappropriately high left ventricular mass in asymptomatic severe aortic stenosis. Heart. 2011;97:301–7. - PubMed
-
- Rajappan K, Rimoldi OE, Dutka DP, Ariff B, Pennell DJ, Sheridan DJ, Camici PG. Mechanisms of coronary microcirculatory dysfunction in patients with aortic stenosis and angiographically normal coronary arteries. Circulation. 2002;105:470–6. - PubMed
-
- Beach JM, Mihaljevic T, Rajeswaran J, Marwick T, Edwards ST, Nowicki ER, Thomas J, Svensson LG, Griffin B, Gillinov AM, Blackstone EH. Ventricular hypertrophy and left atrial dilatation persist and are associated with reduced survival after valve replacement for aortic stenosis. J Thorac Cardiovasc Surg. 2014;147:362–9. - PubMed
-
- Cortigiani L, Rigo F, Gherardi S, Bovenzi F, Molinaro S, Picano E, Sicari R. Coronary flow reserve during dipyridamole stress echocardiography predicts mortality. JACC Cardiovasc Imaging. 2012;5:1079–85. - PubMed
-
- Lee H, Park JB, Yoon YE, Park EA, Kim HK, Lee W, Kim YJ, Cho GY, Sohn DW, Greiser A, Lee SP. Noncontrast Myocardial T1 Mapping by Cardiac Magnetic Resonance Predicts Outcome in Patients With Aortic Stenosis. JACC Cardiovasc Imaging. 2018;11:974–83. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials