

Establishment of a new practical telesurgical platform using the hinotori™ Surgical Robot System: a preclinical study
- PMID: 36239792
- PMCID: PMC9562055
- DOI: 10.1007/s00423-022-02710-6
Establishment of a new practical telesurgical platform using the hinotori™ Surgical Robot System: a preclinical study
Abstract
Aim: The recent development of new surgical robots and network telecommunication technology has opened new avenues for robotic telesurgery. Although a few gastroenterological surgeries have been performed in the telesurgery setting, more technically demanding procedures including gastrectomy with D2 lymphadenectomy and intracorporeal anastomosis have never been reported. We examined the feasibility of telesurgical robotic gastrectomy using the hinotori™ Surgical Robot System in a preclinical setting.
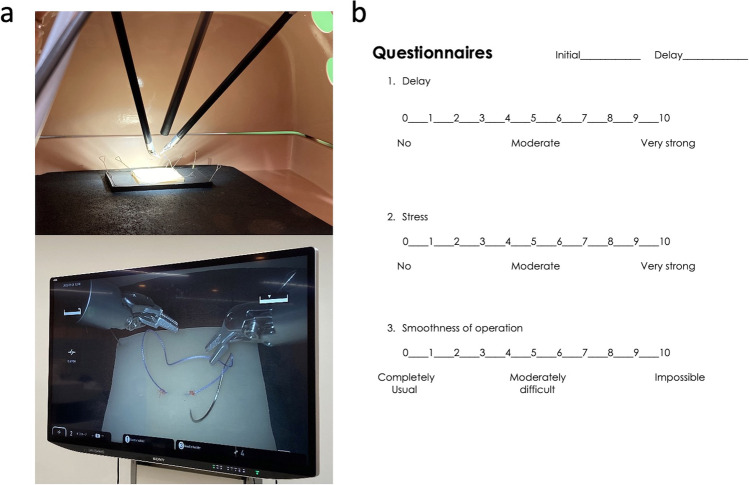
Methods: First, the suturing time in the dry model was measured in the virtual telesurgery setting to determine the latency time threshold. Second, a surgeon cockpit and a patient unit were installed at Okazaki Medical Center and Fujita Health University, respectively (approximately 30 km apart), and connected using a 10-Gbps leased optic-fiber network. After evaluating the feasibility in the dry gastrectomy model, robotic distal gastrectomies with D2 lymphadenectomy and intracorporeal B-I anastomosis were performed in two porcine models.
Results: The virtual telesurgery study identified a latency time threshold of 125 ms. In the actual telesurgery setting, the latency time was 27 ms, including a 2-ms telecommunication network delay and a 25-ms local information process delay. After verifying the feasibility of the operative procedures using a gastrectomy model, two telesurgical gastrectomies were successfully completed without any unexpected events. No fluctuation was observed across the actual telesurgeries.
Conclusion: Short-distance telesurgical robotic surgery for technically more demanding procedure may be safely conducted using the hinotori Surgical Robot System connected by high-speed optic-fiber communication.
Keywords: Gastrectomy; Lymphadenectomy; Remote operations; Robotic surgical procedure.
© 2022. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
Tsuyoshi Tanaka and Ichiro Uyama belong to an endowed chair by Medicaroid Inc. Koichi Suda was funded by Sysmex, Co. in relation to the Collaborative Laboratory for Research and Development in Advanced Surgical Intelligence, Fujita Health University. Koichi Suda has served on advisory boards for Medicaroid Inc. Ichiro Uyama has served on advisory boards for Intuitive Surgical Inc. and has received lecture fees from Intuitive Surgical Inc. and Medicaroid Inc. Masaya Nakauchi, Kenichi Nakamura, Susumu Shibasaki, Kazuki Inaba, Tatsuhiko Harada, Masanao Ohashi, Masayuki Ohigashi, Hiroaki Kitatsuji, Shingo Akimoto, and Kenji Kikuchi have no relevant or material financial interests to disclose.
There is no funding support to be disclosed in this study. Tsuyoshi Tanaka and Ichiro Uyama belong to an endowed chair by Medicaroid Inc. Koichi Suda was funded by Sysmex, Co. in relation to the Collaborative Laboratory for Research and Development in Advanced Surgical Intelligence, Fujita Health University. Koichi Suda has served on advisory boards for Medicaroid Inc. Ichiro Uyama has served on advisory boards for Intuitive Surgical Inc. and has received lecture fees from Intuitive Surgical Inc. and Medicaroid Inc. Masaya Nakauchi, Kenichi Nakamura, Susumu Shibasaki, Kazuki Inaba, Tatsuhiko Harada, Masanao Ohashi, Masayuki Ohigashi, Hiroaki Kitatsuji, Shingo Akimoto, and Kenji Kikuchi have no relevant or material financial interests to disclose.
Figures






References
-
- Anvari M, McKinley C, Stein H. Establishment of the world’s first telerobotic remote surgical service: for provision of advanced laparoscopic surgery in a rural community. Ann Surg. 2005;241:460–464. doi: 10.1097/01.sla.0000154456.69815.ee. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
