

A tale of two unconventional adult diaphragmatic hernias
- PMID: 36239968
- PMCID: PMC10149238
- DOI: 10.1308/rcsann.2022.0107
A tale of two unconventional adult diaphragmatic hernias
Abstract
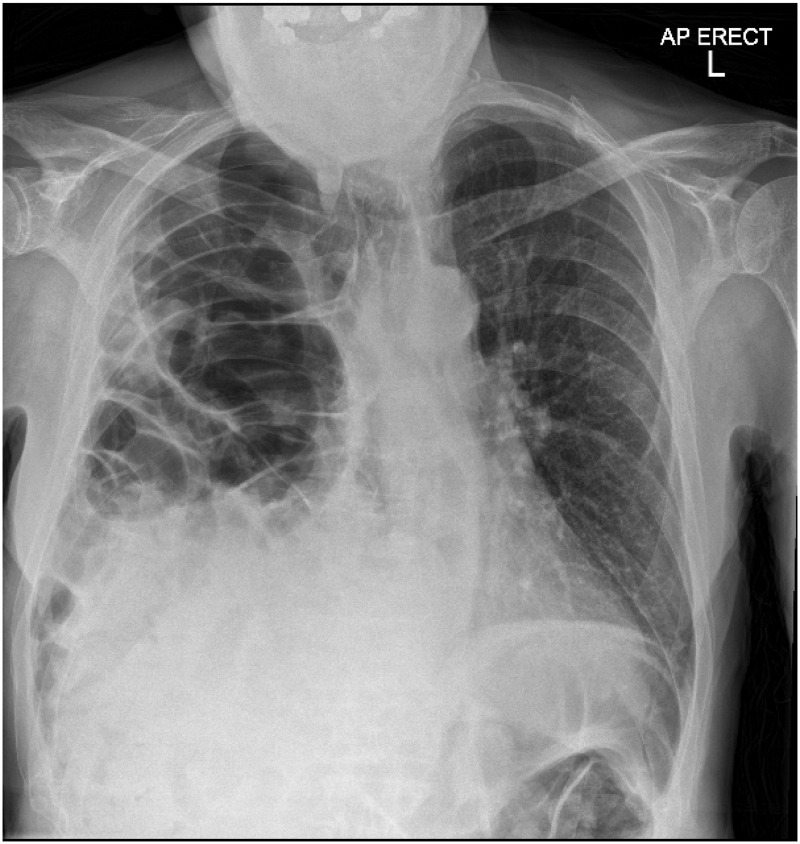
Diaphragmatic hernias can be congenital or acquired and are a protrusion of intra-abdominal contents through an abnormal opening in the diaphragm. Acquired defects are rare and occur secondary to direct penetrating injury or blunt abdominal trauma. This case review demonstrates two unconventional cases of large diaphragmatic hernias with viscero-abdominal disproportion in adults. Case 1 is a 27-year-old man with no prior medical or surgical history. He presented following a 24-h history of increasing shortness of breath and left-sided pleuritic chest pain, and no history of trauma. Chest X-ray demonstrated loops of bowel within the left hemithorax with displacement of the mediastinum to the right. Computed tomography (CT) scan confirmed a large diaphragmatic defect causing herniation of most of his abdominal contents into the left hemithorax. He underwent emergency surgery, which confirmed the viscero-abdominal disproportion. He required an extended right hemicolectomy to reduce the volume of the abdominal comtents and laparostomy to reduce the risk of abdominal compartment syndrome and recurrence of the hernia. Case 2 is a 76-year-old man with significant medical comorbidities who presented with acute onset of abdominal pain. He had a history of traumatic right-sided chest injury as a child resulting in right-sided diaphragmatic paralysis. Chest X-ray demonstrated a large right-sided diaphragmatic hernia with abdominal viscera in the right thoracic cavity. CT scan of the chest, abdomen and pelvis demonstrated both small and large bowel loops within the right hemithorax, compression of the right lung and displacement of the mediastinum to the left. The CT scan also demonstarted viscero-abdominal disproportion. Operative management was considered initially but following improvement with basic medical management and no further deterioration, a non-operative approach was adopted. Both cases illustrate atypical presentations of adults with diaphragmatic hernias. In an ideal scenario, these are repaired surgically. When the presumed diagnosis shows characteristics of a viscero-abdominal disproportion and surgery is pursued, the surgeon must consider that primary abdominal closure may not be possible and multiple operations may be necessary to correct the defect and achieve closure. Sacrifice of abdominal viscera may also be necessary to reduce the volume of abdominal contents.
Keywords: Abdominal compartment syndrome; Blunt and penetrating trauma; Congenital diaphragmatic hernia; Delayed closure; Diaphragmatic hernia; Open and minimal access repair; Viscero-abdominal disproportion.
Figures




Similar articles
-
Right-sided strangulating diaphragmatic hernia in an adult without history of trauma: a case report.J Med Case Rep. 2021 Jul 13;15(1):372. doi: 10.1186/s13256-021-02861-y. J Med Case Rep. 2021. PMID: 34256846 Free PMC article.
-
Symptomatic congenital Morgagni hernia presenting as a chest pain: a case report.J Med Case Rep. 2020 Jan 18;14(1):13. doi: 10.1186/s13256-019-2336-9. J Med Case Rep. 2020. PMID: 31952551 Free PMC article.
-
Intra-thoracic Symptomatic Gallstones in a Right-Sided Post-traumatic Diaphragmatic Hernia: A Case Report.Cureus. 2022 Dec 22;14(12):e32824. doi: 10.7759/cureus.32824. eCollection 2022 Dec. Cureus. 2022. PMID: 36699800 Free PMC article.
-
Non traumatic right Bochdalek hernia with loss of Domain in adults. Our experience and review of literature.Ann Ital Chir. 2023 Sep 5;12:S2239253X23039877. Ann Ital Chir. 2023. PMID: 37814503 Review.
-
Emergency surgery due to diaphragmatic hernia: case series and review.World J Emerg Surg. 2017 May 18;12:23. doi: 10.1186/s13017-017-0134-5. eCollection 2017. World J Emerg Surg. 2017. PMID: 28529538 Free PMC article. Review.
Cited by
-
Area of Focus in 3D Volumetry and Botulinum Toxin A Injection for Giant Diaphragmatic Hernia with Loss of Domain: A Case Report with Video Illustration.J Abdom Wall Surg. 2024 Sep 6;3:13448. doi: 10.3389/jaws.2024.13448. eCollection 2024. J Abdom Wall Surg. 2024. PMID: 39310670 Free PMC article.
-
Diaphragmatic Hernia Repair in Adult Patients: A Retrospective Institutional Experience.Cureus. 2024 Nov 27;16(11):e74601. doi: 10.7759/cureus.74601. eCollection 2024 Nov. Cureus. 2024. PMID: 39734943 Free PMC article.
-
Nontraumatic right diaphragmatic hernia with malrotated left liver lobe incarceration: An unusual case report with literature review.Radiol Case Rep. 2024 Dec 30;20(3):1610-1614. doi: 10.1016/j.radcr.2024.12.015. eCollection 2025 Mar. Radiol Case Rep. 2024. PMID: 39845283 Free PMC article.
References
-
- Amboss. Acquired Diaphragmatic Hernias. http://www.amboss.com/us/knowledge/Acquired_diaphragmatic_hernias/ (cited April 2023).
-
- Maxwell D, Baird R, Puligandla P. Abdominal wall closure in neonates after congenital diaphragmatic hernia repair. J Pediatr Surg 2013; 48: 930–934. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources