

Pilot clinical and pharmacokinetic study of Δ9-Tetrahydrocannabinol (THC)/Cannabidiol (CBD) nanoparticle oro-buccal spray in patients with advanced cancer experiencing uncontrolled pain
- PMID: 36240167
- PMCID: PMC9565400
- DOI: 10.1371/journal.pone.0270543
Pilot clinical and pharmacokinetic study of Δ9-Tetrahydrocannabinol (THC)/Cannabidiol (CBD) nanoparticle oro-buccal spray in patients with advanced cancer experiencing uncontrolled pain
Abstract
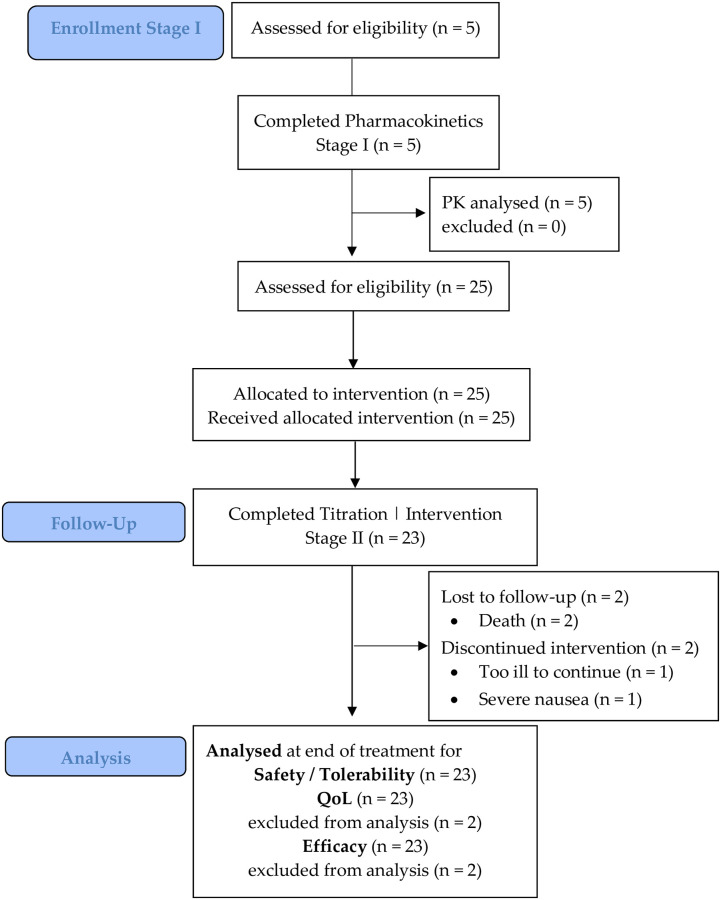
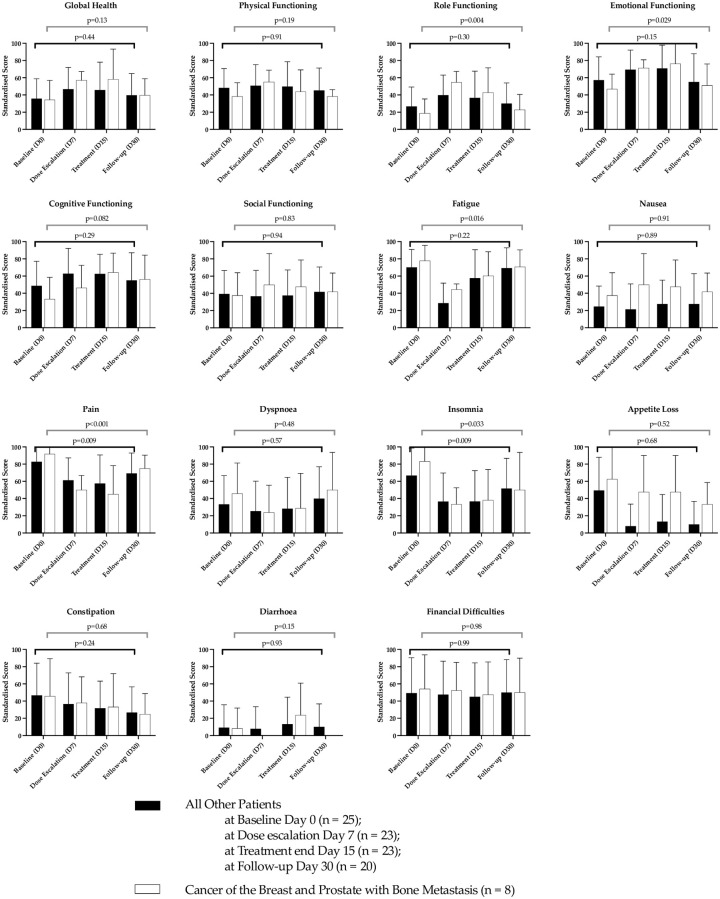
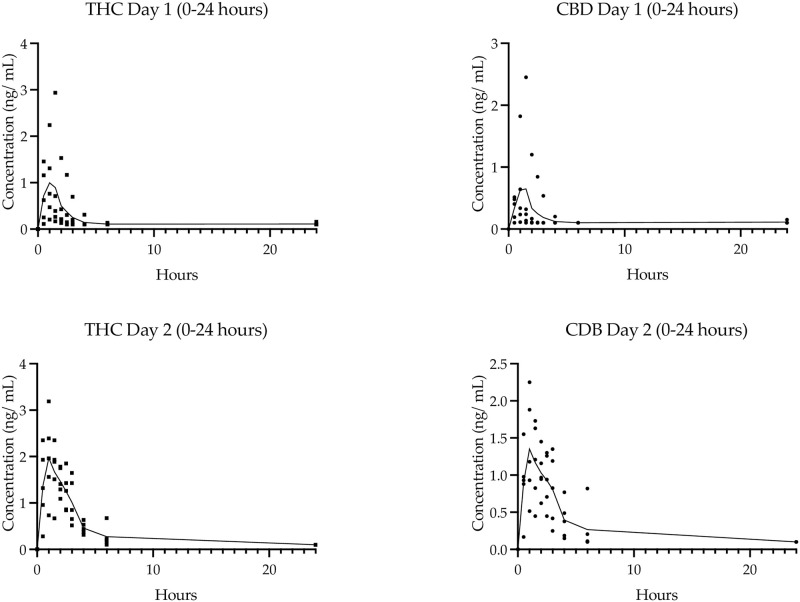
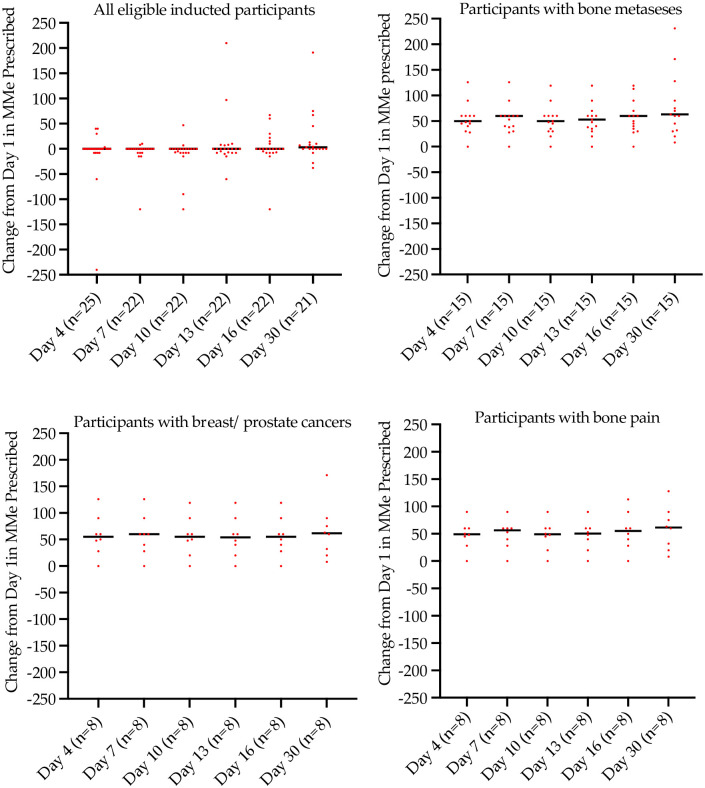
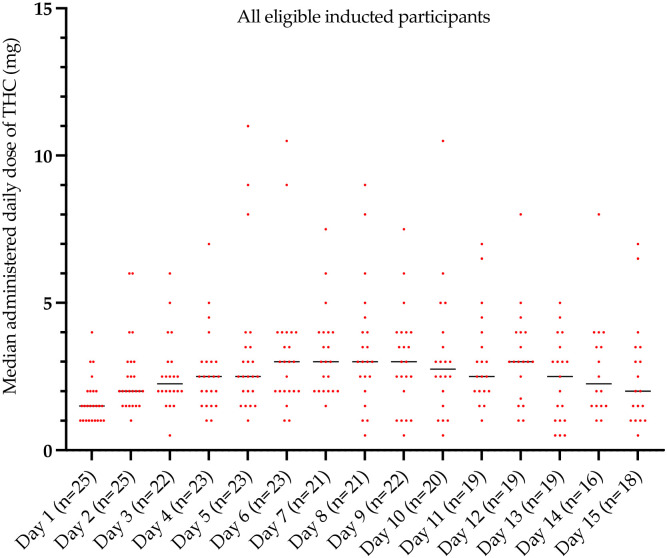
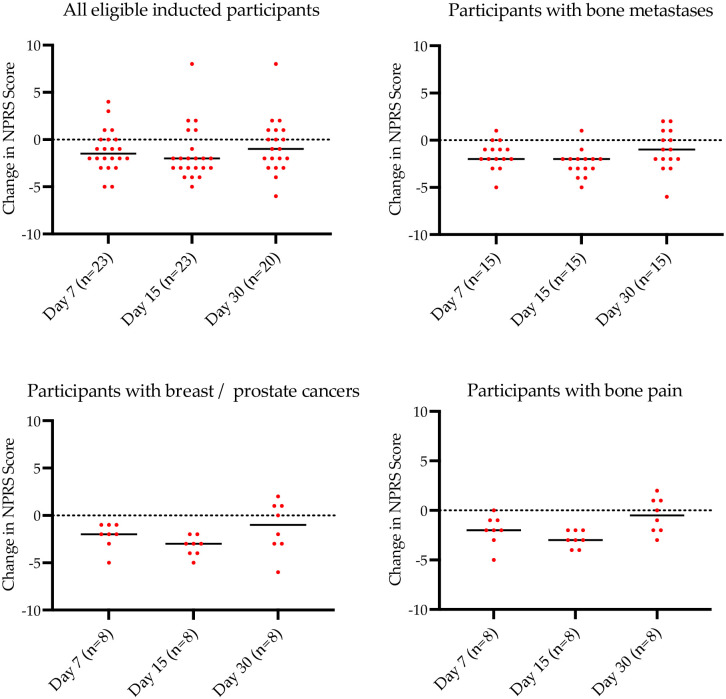
This pilot study aimed to assess the safety, tolerability, pharmacokinetics and exploratory analgesic effect of a novel water-soluble oro-buccal nanoparticle spray of a cannabis-based medicine (MDCNS-01) in patients with advanced incurable malignancy with unrelieved pain from opioid analgesic. The study was a non-blinded single arm 2 stage study. Stage I was a single escalating dose (n = 5) [2.5 mg Δ9-THC and 2.5 mg CBD) versus a 3-fold escalated dose. Stage II was an up-titrated dose in patients with advanced cancers and intractable pain (n = 25). During Stage I with an increased cannabis-based medicine dose, maximum observed plasma concentrations of cannabinoids were dose dependant. The water-soluble formulation in the current study resulted in a higher median (min, max) systemic exposure of Δ9-THC than CBD (AUC from 2.5 mg each of Δ9-THC and CBD, was 1.71 ng mL.h-1 (1.1, 6.6) and 0.65 ng mL.h-1 (0.49, 4.1), respectively). During stage II a subgroup of patients diagnosed with breast and prostate cancers with bone metastases, had the highest mean pain score improvement from baseline of 40% (unadjusted) and 33% (adjusted for rescue medication use). For all patients the most reported adverse events were mild or moderate drowsiness affecting 11 (44%) and 4 (6%) patients, respectively, and nausea and vomiting that affected 18 (72%) patients. The water-soluble cannabis-based medicine provided acceptable bioavailability for Δ9-THC/CBD, appeared safe and tolerable in advanced incurable cancers with uncontrolled pain with preliminary evidence of analgesic efficacy.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests, SC, AJM are consultants for Medlab Clinical, and BB was contracted by the funder to carry out an independent overall analysis of the data. JDH, DR, SH, LV own shares in Medlab Clinical and participate in its cannabis-based medicines research programs and the pilot clinical trial administered formulation, MDCNB-01 (NanaBisTM). Medlab Clinical also has granted patents for its submicron particle technology in all global western regions. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
An open-label extension study to investigate the long-term safety and tolerability of THC/CBD oromucosal spray and oromucosal THC spray in patients with terminal cancer-related pain refractory to strong opioid analgesics.J Pain Symptom Manage. 2013 Aug;46(2):207-18. doi: 10.1016/j.jpainsymman.2012.07.014. Epub 2012 Nov 8. J Pain Symptom Manage. 2013. PMID: 23141881 Clinical Trial.
-
A pilot safety, tolerability and pharmacokinetic study of an oro-buccal administered cannabidiol-dominant anti-inflammatory formulation in healthy individuals: a randomized placebo-controlled single-blinded study.Inflammopharmacology. 2021 Oct;29(5):1361-1370. doi: 10.1007/s10787-021-00859-y. Epub 2021 Aug 6. Inflammopharmacology. 2021. PMID: 34357480 Clinical Trial.
-
Urinary Pharmacokinetic Profile of Cannabidiol (CBD), Δ9-Tetrahydrocannabinol (THC) and Their Metabolites following Oral and Vaporized CBD and Vaporized CBD-Dominant Cannabis Administration.J Anal Toxicol. 2022 May 20;46(5):494-503. doi: 10.1093/jat/bkab059. J Anal Toxicol. 2022. PMID: 34089060 Free PMC article.
-
Nanomaterials-Based Electrochemical Δ9-THC and CBD Sensors for Chronic Pain.Biosensors (Basel). 2023 Mar 14;13(3):384. doi: 10.3390/bios13030384. Biosensors (Basel). 2023. PMID: 36979596 Free PMC article. Review.
-
Antinociceptive effects of minor cannabinoids, terpenes and flavonoids in Cannabis.Behav Pharmacol. 2022 Apr 1;33(2&3):130-157. doi: 10.1097/FBP.0000000000000627. Behav Pharmacol. 2022. PMID: 33709984 Review.
Cited by
-
How to ESCAPE from Pain? An Observational Study on Improving Pain and Quality of Life with the Cannamedical® Hybrid Cannabis Extract.Adv Ther. 2025 Jun 25. doi: 10.1007/s12325-025-03262-z. Online ahead of print. Adv Ther. 2025. PMID: 40560527
-
Cannabinoids in Treating Chemotherapy-Induced Nausea and Vomiting, Cancer-Associated Pain, and Tumor Growth.Int J Mol Sci. 2023 Dec 20;25(1):74. doi: 10.3390/ijms25010074. Int J Mol Sci. 2023. PMID: 38203245 Free PMC article. Review.
-
Medicinal Cannabis and the Intestinal Microbiome.Pharmaceuticals (Basel). 2024 Dec 17;17(12):1702. doi: 10.3390/ph17121702. Pharmaceuticals (Basel). 2024. PMID: 39770543 Free PMC article. Review.
-
Adverse events associated with the use of cannabis-based products in people living with cancer: a systematic scoping review.Support Care Cancer. 2024 Dec 18;33(1):40. doi: 10.1007/s00520-024-09087-w. Support Care Cancer. 2024. PMID: 39694905 Free PMC article.
-
CBD and THC in Special Populations: Pharmacokinetics and Drug-Drug Interactions.Pharmaceutics. 2024 Apr 1;16(4):484. doi: 10.3390/pharmaceutics16040484. Pharmaceutics. 2024. PMID: 38675145 Free PMC article. Review.
References
-
- Aviram J, Samuelly-Leichtag G. Efficacy of Cannabis-Based Medicines for Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pain Physician. 2017;20(6):E755–e96. Epub 2017/09/22. . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
