

Predictive validity of the quick Sequential Organ Failure Assessment (qSOFA) score for the mortality in patients with sepsis in Vietnamese intensive care units
- PMID: 36240177
- PMCID: PMC9565713
- DOI: 10.1371/journal.pone.0275739
Predictive validity of the quick Sequential Organ Failure Assessment (qSOFA) score for the mortality in patients with sepsis in Vietnamese intensive care units
Abstract
Background: The simple scoring systems for predicting the outcome of sepsis in intensive care units (ICUs) are few, especially for limited-resource settings. Therefore, this study aimed to evaluate the accuracy of the quick Sequential (Sepsis-Related) Organ Failure Assessment (qSOFA) score in predicting the mortality of ICU patients with sepsis in Vietnam.
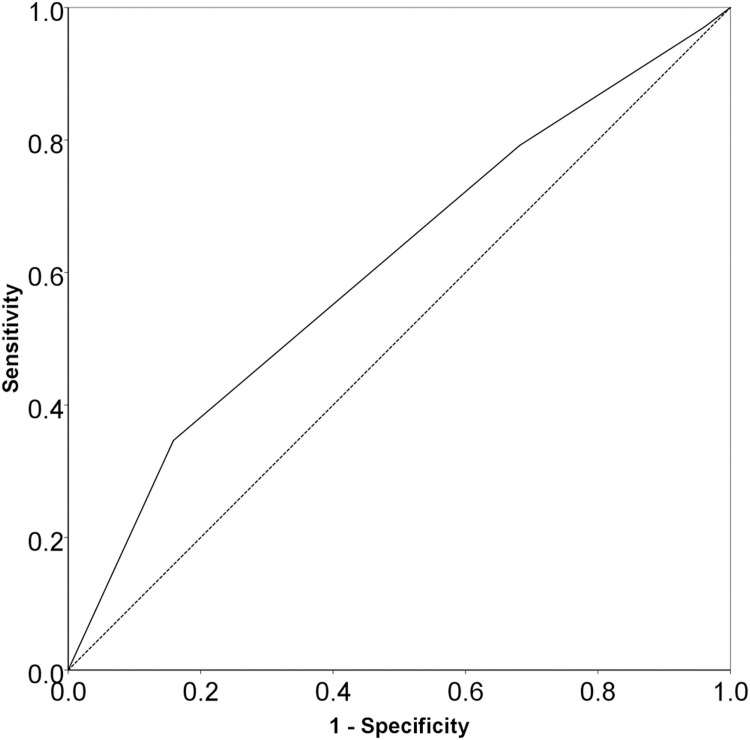
Methods: We did a multicenter cross-sectional study of patients with sepsis (≥18 years old) presenting to 15 adult ICUs throughout Vietnam on the specified days (i.e., 9th January, 3rd April, 3rd July, and 9th October) representing the different seasons of 2019. The primary and secondary outcomes were the hospital and ICU all-cause mortalities, respectively. The area under the receiver operating characteristic curve (AUROC) was calculated to determine the discriminatory ability of the qSOFA score for deaths in the hospital and ICU. The cut-off value of the qSOFA scores was determined by the receiver operating characteristic curve analysis. Upon ICU admission, factors associated with the hospital and ICU mortalities were assessed in univariable and multivariable logistic models.
Results: Of 252 patients, 40.1% died in the hospital, and 33.3% died in the ICU. The qSOFA score had a poor discriminatory ability for both the hospital (AUROC: 0.610 [95% CI: 0.538 to 0.681]; cut-off value: ≥2.5; sensitivity: 34.7%; specificity: 84.1%; PAUROC = 0.003) and ICU (AUROC: 0.619 [95% CI: 0.544 to 0.694]; cutoff value: ≥2.5; sensitivity: 36.9%; specificity: 83.3%; PAUROC = 0.002) mortalities. However, multivariable logistic regression analyses show that the qSOFA score of 3 was independently associated with the increased risk of deaths in both the hospital (adjusted odds ratio, AOR: 3.358; 95% confidence interval, CI: 1.756 to 6.422) and the ICU (AOR: 3.060; 95% CI: 1.651 to 5.671).
Conclusion: In our study, despite having a poor discriminatory value, the qSOFA score seems worthwhile in predicting mortality in ICU patients with sepsis in limited-resource settings.
Clinical trial registration: Clinical trials registry-India: CTRI/2019/01/016898.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Rudd KE, Johnson SC, Agesa KM, Shackelford KA, Tsoi D, Kievlan DR, et al.. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet. 2020;395(10219):200–11. Epub 2020/01/20. doi: 10.1016/S0140-6736(19)32989-7 ; PubMed Central PMCID: PMC6970225. - DOI - PMC - PubMed
-
- Bauer M, Gerlach H, Vogelmann T, Preissing F, Stiefel J, Adam D. Mortality in sepsis and septic shock in Europe, North America and Australia between 2009 and 2019- results from a systematic review and meta-analysis. Critical care (London, England). 2020;24(1):239. Epub 2020/05/21. doi: 10.1186/s13054-020-02950-2 ; PubMed Central PMCID: PMC7236499. - DOI - PMC - PubMed
-
- Phua J, Koh Y, Du B, Tang YQ, Divatia JV, Tan CC, et al.. Management of severe sepsis in patients admitted to Asian intensive care units: prospective cohort study. Bmj. 2011;342:d3245. Epub 2011/06/15. doi: 10.1136/bmj.d3245 ; PubMed Central PMCID: PMC3113333 www.icmje.org/coi_disclosure.pdf. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
