

Adherence to multidisciplinary care in a prospective chronic kidney disease cohort is associated with better outcomes
- PMID: 36240220
- PMCID: PMC9565398
- DOI: 10.1371/journal.pone.0266617
Adherence to multidisciplinary care in a prospective chronic kidney disease cohort is associated with better outcomes
Abstract
Introduction: The Renal Healthcare Program Uruguay (NRHP-UY) is a national, multidisciplinary program that provides care to chronic kidney disease (CKD) patients. In this study, we report the global results of CKD patient outcomes and a comparison between those treated at the NRHP-UY Units, with those patients who were initially included in the program but did not adhere to follow up.
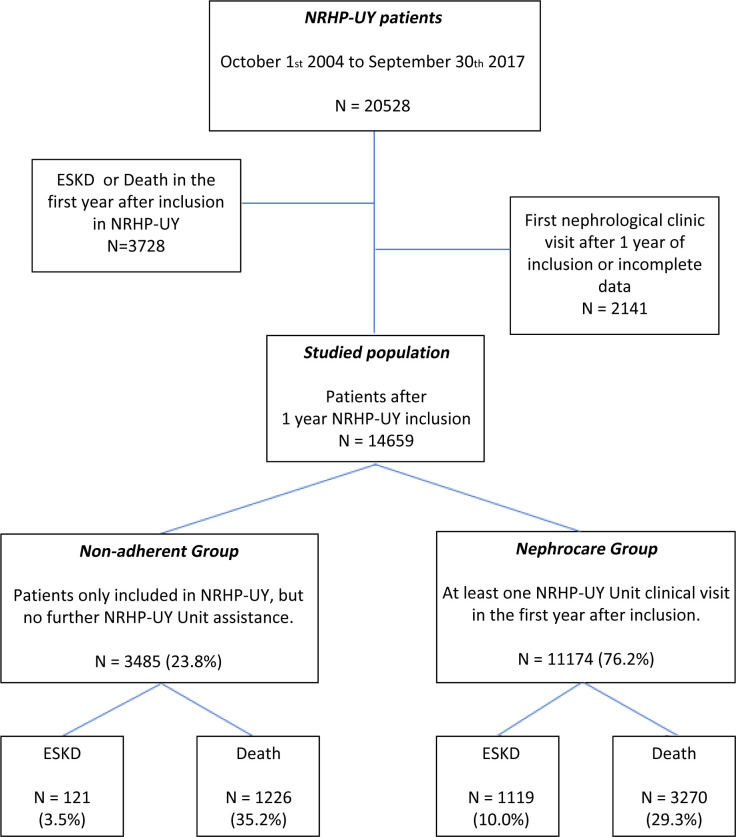
Methods: A cohort of not-on dialysis CKD patients included prospectively in the NRHP-UY between October 1st 2004 and September 30th 2017 was followed-up until September 30th 2019. Two groups were compared: a) Nephrocare Group: Patients who had at least one clinic visit during the first year on NRHP-UY (n = 11174) and b) Non-adherent Group: Patients who were informed and accepted to be included but had no subsequent data registered after admission (n = 3485). The study was approved by the Ethics Committee and all patients signed an informed consent. Outcomes were studied with Logistic and Cox´s regression analysis, Fine and Gray competitive risk and propensity-score matching tests.
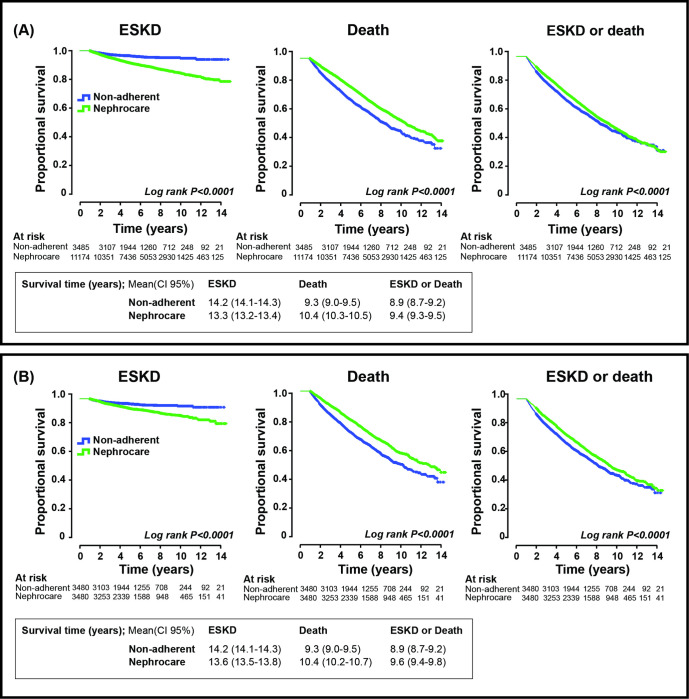
Results: 14659 patients were analyzed, median age 70 (60-77) years, 56.9% male. The Nephrocare Group showed improved achievement of therapeutic goals, ESKD was more frequent (HR 2.081, CI 95%1.722-2.514) as planned kidney replacement therapy (KRT) start (OR 2.494, CI95% 1.591-3.910), but mortality and the combined event (death and ESKD) were less frequent (HR 0.671, CI95% 0.628-0.717 and 0.777, CI95% 0.731-0.827) (p = 0.000) compared to the Non-adherent group. Results were similar in the propensity-matched group: ESKD (HR 2.041, CI95% 1.643-2.534); planned kidney replacement therapy (KRT) start (OR 2.191, CI95% 1.322-3.631) death (HR 0.692, CI95% 0.637-0.753); combined event (HR 0.801, CI95% 0.742-0.865) (p = 0.000).
Conclusion: Multidisciplinary care within the NRHP-UY is associated with timely initiation of KRT and lower mortality in single outcomes, combined analysis, and propensity-matched analysis.
Conflict of interest statement
The authors have declared that no competing interests exist
Figures
References
-
- Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Hypertension 2003; 42: 1050–1065. doi: 10.1161/01.HYP.0000102971.85504.7c - DOI - PubMed
-
- Willis K, Cheung M, Slifer S. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2013;3(1):Supplement. 3. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
