

Quantitative epileptiform burden and electroencephalography background features predict post-traumatic epilepsy
- PMID: 36241423
- PMCID: PMC9931627
- DOI: 10.1136/jnnp-2022-329542
Quantitative epileptiform burden and electroencephalography background features predict post-traumatic epilepsy
Abstract
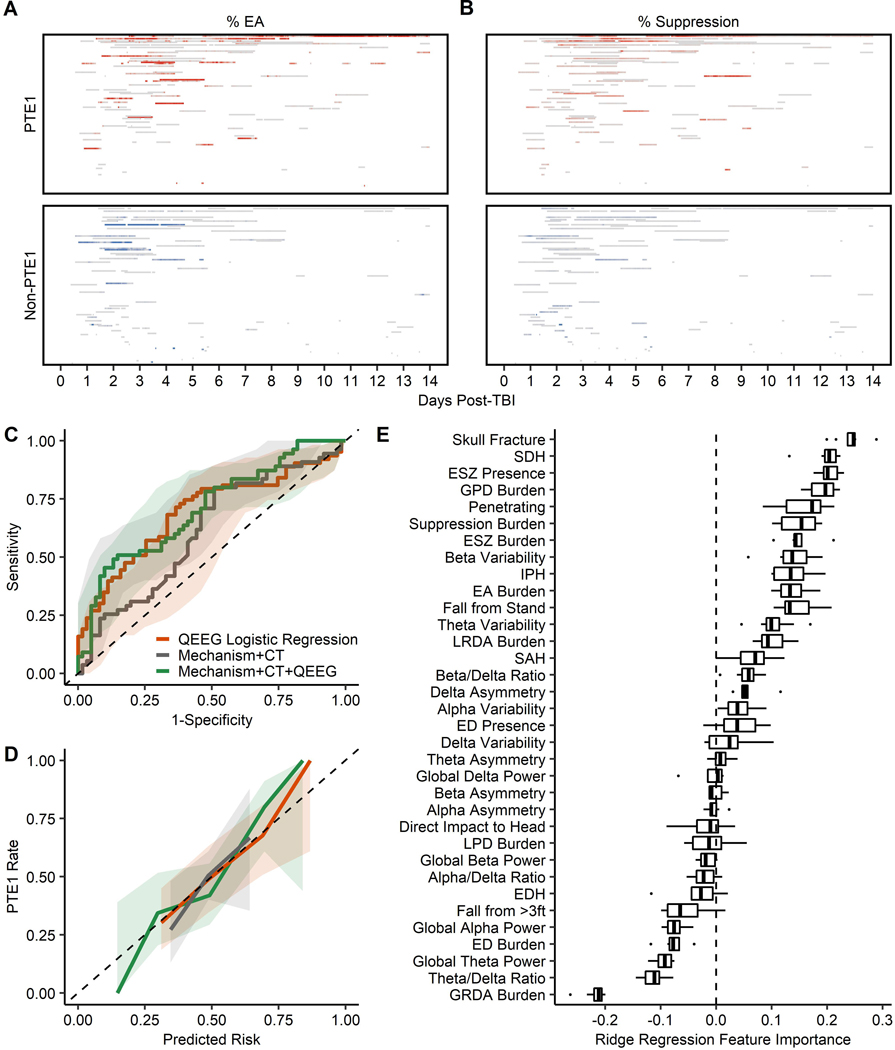
Background: Post-traumatic epilepsy (PTE) is a severe complication of traumatic brain injury (TBI). Electroencephalography aids early post-traumatic seizure diagnosis, but its optimal utility for PTE prediction remains unknown. We aim to evaluate the contribution of quantitative electroencephalograms to predict first-year PTE (PTE1).
Methods: We performed a multicentre, retrospective case-control study of patients with TBI. 63 PTE1 patients were matched with 63 non-PTE1 patients by admission Glasgow Coma Scale score, age and sex. We evaluated the association of quantitative electroencephalography features with PTE1 using logistic regressions and examined their predictive value relative to TBI mechanism and CT abnormalities.
Results: In the matched cohort (n=126), greater epileptiform burden, suppression burden and beta variability were associated with 4.6 times higher PTE1 risk based on multivariable logistic regression analysis (area under the receiver operating characteristic curve, AUC (95% CI) 0.69 (0.60 to 0.78)). Among 116 (92%) patients with available CT reports, adding quantitative electroencephalography features to a combined mechanism and CT model improved performance (AUC (95% CI), 0.71 (0.61 to 0.80) vs 0.61 (0.51 to 0.72)).
Conclusions: Epileptiform and spectral characteristics enhance covariates identified on TBI admission and CT abnormalities in PTE1 prediction. Future trials should incorporate quantitative electroencephalography features to validate this enhancement of PTE risk stratification models.
Keywords: EEG; EPILEPSY; TRAUMATIC BRAIN INJURY.
© Author(s) (or their employer(s)) 2023. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Jennett B, Van De Sande J. EEG prediction of post-traumatic epilepsy. Epilepsia. 1975;16(2):251–256. - PubMed
Publication types
MeSH terms
Grants and funding
- K23 NS110980/NS/NINDS NIH HHS/United States
- R01 NS102190/NS/NINDS NIH HHS/United States
- UL1 TR000064/TR/NCATS NIH HHS/United States
- R01 NS111022/NS/NINDS NIH HHS/United States
- R01 AG073410/AG/NIA NIH HHS/United States
- UL1 TR001427/TR/NCATS NIH HHS/United States
- R34 AG061304/AG/NIA NIH HHS/United States
- R25 NS065743/NS/NINDS NIH HHS/United States
- RF1 NS115268/NS/NINDS NIH HHS/United States
- DP2 HD101400/HD/NICHD NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- UL1 TR002736/TR/NCATS NIH HHS/United States
- RF1 NS120947/NS/NINDS NIH HHS/United States
- R01 NS117904/NS/NINDS NIH HHS/United States
- K23 NS112596/NS/NINDS NIH HHS/United States
- R21 NS128641/NS/NINDS NIH HHS/United States
- R01 HL161253/HL/NHLBI NIH HHS/United States
- F30 NS060325/NS/NINDS NIH HHS/United States
- RF1 AG064312/AG/NIA NIH HHS/United States
- R01 NS102574/NS/NINDS NIH HHS/United States
- R21 NS109627/NS/NINDS NIH HHS/United States
- R01 NS126282/NS/NINDS NIH HHS/United States
- R01 NS107291/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical