

Practice Guideline
doi: 10.1016/j.jacc.2022.08.750.
Epub 2022 Oct 11.
2022 ACC Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department: A Report of the American College of Cardiology Solution Set Oversight Committee
- PMID: 36241466
- PMCID: PMC10691881
- DOI: 10.1016/j.jacc.2022.08.750
Item in Clipboard
Practice Guideline
2022 ACC Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department: A Report of the American College of Cardiology Solution Set Oversight Committee
J Am Coll Cardiol.
.
Erratum in
-
Correction.J Am Coll Cardiol. 2024 Aug 20;84(8):771. doi: 10.1016/j.jacc.2024.07.009. J Am Coll Cardiol. 2024. PMID: 39142734 No abstract available.
No abstract available
Keywords: ACC Expert Consensus Decision Pathway; accelerated diagnostic pathway; acute coronary syndrome; biomarkers; cardiac imaging; chest pain; clinical decision pathway; emergency department; myocardial infarction; myocardial injury; myocardial ischemia; stress test; troponins.
Figures
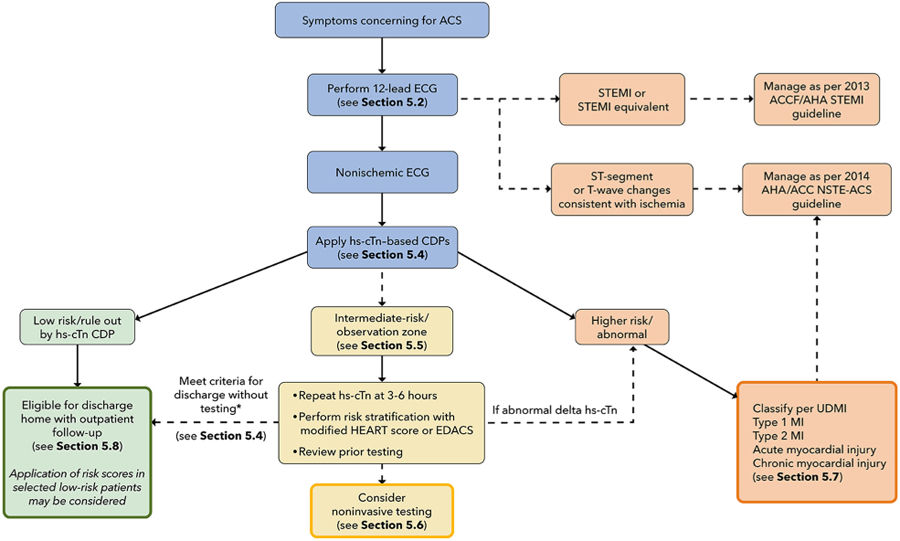
*Unchanged high-sensitivity troponin concentration (ie, no or minimal change over serial measurements) with 1) recent normal testing (ie, invasive or CT coronary angiogram <2 years ago or stress test <1 year ago); 2) symptoms inconsistent with possible ACS; 3) chronic elevations in hs-cTn that are unchanged compared with levels measured previously; or 4) a modified HEART score ≤3 or EDACS <16. ACC = American College Cardiology; ACS = acute coronary syndrome; AHA = American Heart Association; CDP = clinical decision pathway; ECG = electrocardiogram; EDACS = Emergency Department Assessment of Chest Pain Score; HEART = History, ECG, Age, Risk Factors, and Troponin; hs-cTn = high-sensitivity cardiac troponin; MI = myocardial infarction; NSTE-ACS = non-ST-segment elevation acute coronary syndrome; STEMI = ST-segment elevation myocardial infarction; UDMI = Universal Definition of MI.
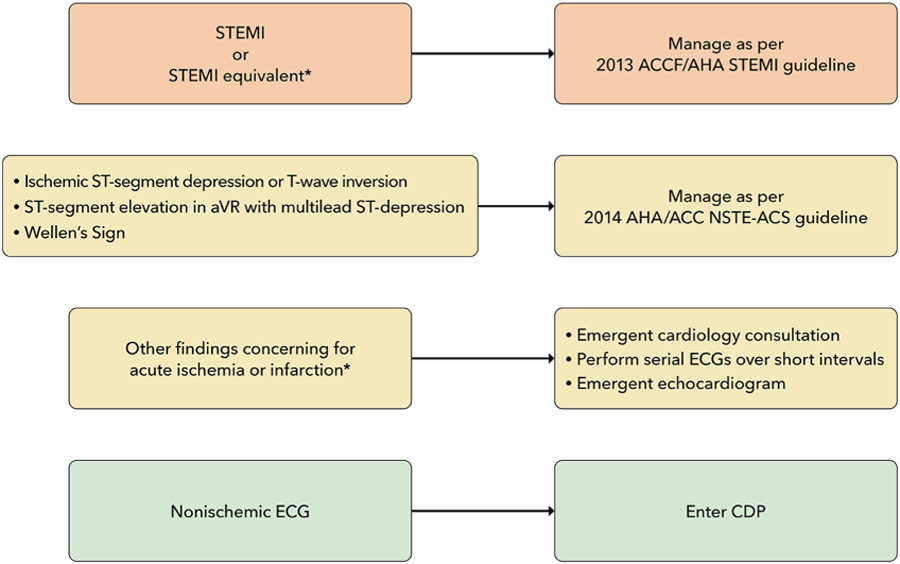
*See Table 1 for ECG findings of STEMI equivalent and findings consistent with ischemia or infarction. ACC = American College of Cardiology; AHA = American Heart Association; aVR = augmented vector right; CDP = clinical decision pathway; ECG = electrocardiogram; NSTE-ACS = non–ST-segment elevation acute coronary syndrome; STEMI = ST-segment elevation myocardial infarction.
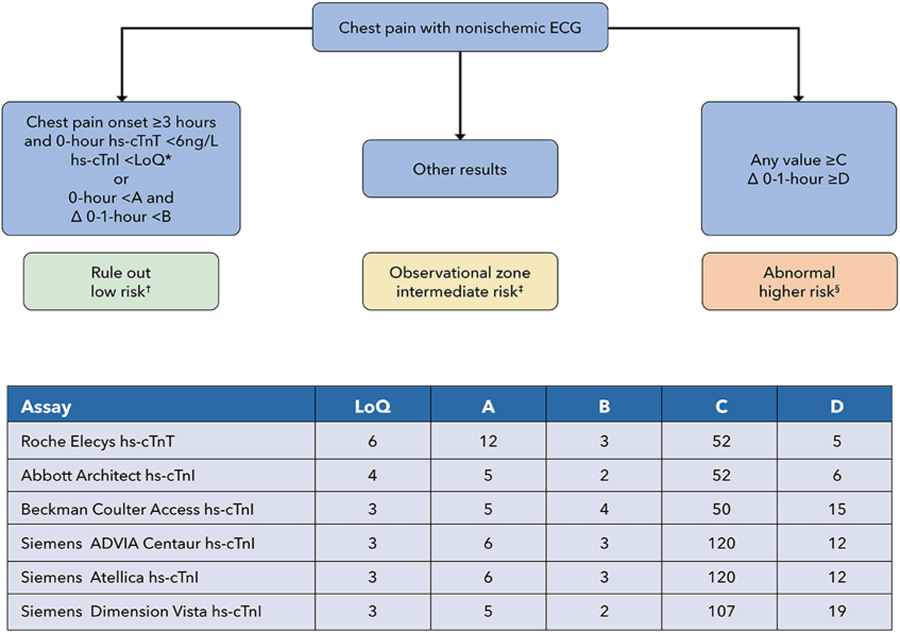
Sources for this Figure: ,,–,– Note that variations of these rapid CDPs have been implemented in different centers, and modification of the algorithms shown may be considered based on local considerations. All values in the chart in are ng/L. *The LoQ may differ slightly from the 0-hour rule-out threshold tested in individual studies. Using a cutoff of <5 ng/L can also be considered instead of the LoQ for the 0-hour rule-out threshold for hs-cTnI assays. †See Sections 5.6 and 5.8 for recommendations on follow-up and testing. ‡See Section 5.5.3. Additional evaluation should include at least one additional observation with hs-cTn measurement at 3–6 hours, with classification of myocardial injury, as described in Section 5.7, into chronic myocardial injury, acute myocardial injury, type 1 MI, and type 2 MI, as per the Universal Definition of Myocardial Infarction. §Patients with acute MI should be managed according to standard practice guidelines. CDP = clinical decision pathway; ECG = electrocardiogram; hs-cTnI= high-sensitivity cardiac troponin I; hs-cTnT = high-sensitivity cardiac troponin T; LoQ = limit of quantification; MI = myocardial infarction.
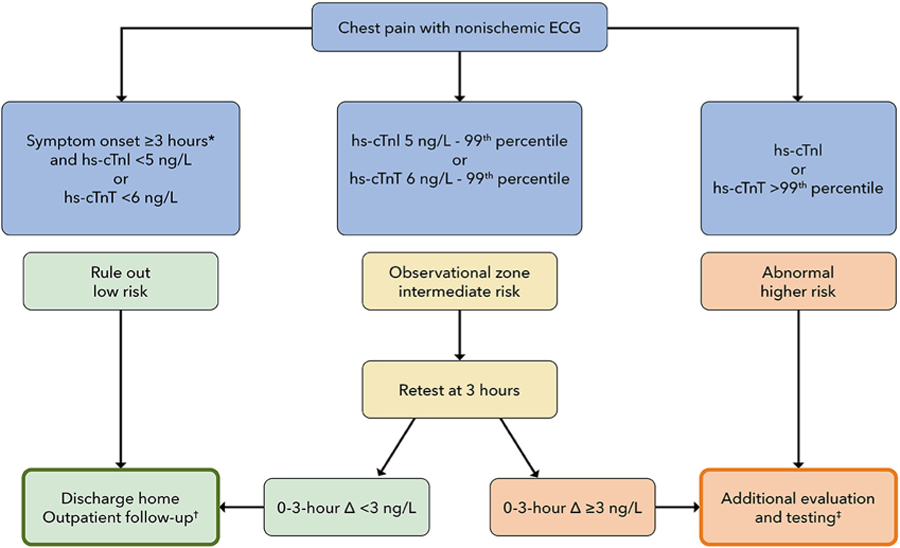
Sources for this Figure: , *Although clinical trials with the HIGH-STEACS pathway have required chest pain onset ≥2 hours before presentation, we recommend requiring a ≥3-hour period between chest pain onset and the first troponin measurement in order to qualify for rule out at time 0. †See Sections 5.6 and 5.8 for recommendations on outpatient follow-up and testing. ‡Additional evaluation is recommended, with consideration of hospital observation or admission, and noninvasive anatomical or functional testing as described in Section 5.6. Myocardial injury should be classified as described in Section 5.7 into chronic myocardial injury, acute myocardial injury, type 1 MI, and type 2 MI, as per the Universal Definition of Myocardial Infarction. Patients with acute MI should be managed according to standard practice guidelines. Patients with chronic myocardial injury may be appropriate for discharge and management in an outpatient setting (see Sections 5.7 and 5.8). ACS = acute coronary syndrome; ECG = electrocardiogram; High-STEACS = High-Sensitivity Troponin in the Evaluation of Patients With Acute Coronary Syndrome; hs-cTnI = high-sensitivity cardiac troponin I; hs-cTnT = high-sensitivity cardiac troponin T; MI = myocardial infarction.
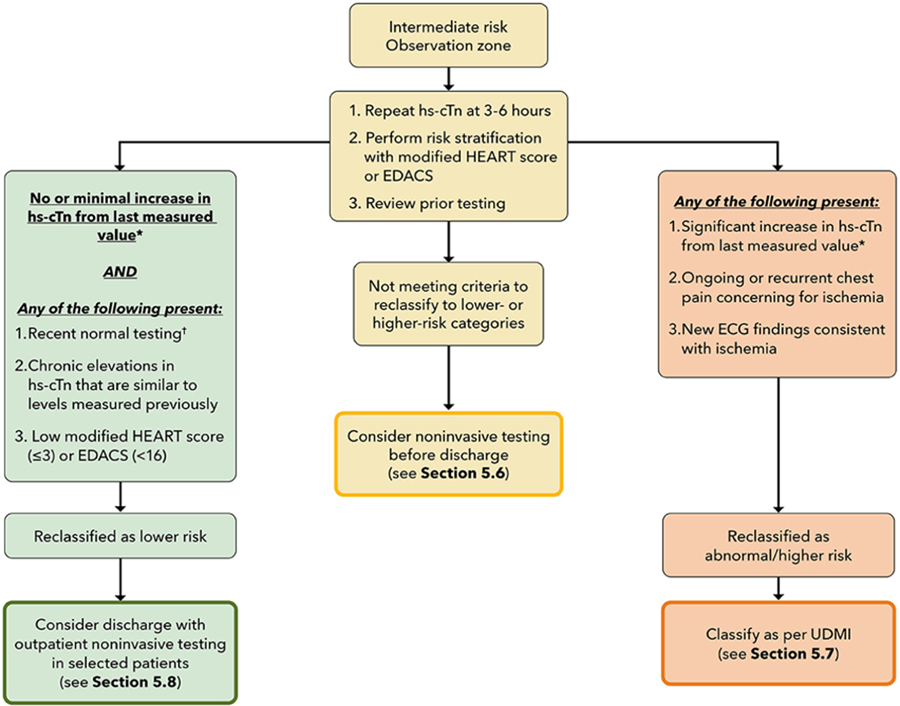
*Evidence-based criteria do not exist to define change thresholds for hs-cTn at the 3- to 6-hour timepoint. As reviewed in Section 5.2, although a 20% relative change from the baseline measurement has been proposed to define significant change, this threshold lacks specificity at low hs-cTn values in part due to assay imprecision. Thus, at lower hs-cTn values near the sex-specific 99th percentile URL values, absolute changes should be used to define clinically-significant change, whereas at higher troponin values, a 20% relative change in values may be a more reasonable threshold. Clinical judgment is needed to interpret small fluctuations in hs-cTn values over serial measurements, as these small changes may reflect assay imprecision rather than acute cardiac injury. †Recent normal testing is considered an invasive or CT coronary angiogram <2 years without evidence of coronary plaque or a stress test <1 year without ischemia. ECG = electrocardiogram; EDACS = Emergency Department Assessment of Chest Pain Score; HEART = History, ECG, Age, Risk Factors, and Troponin; hs-cTn = high-sensitivity cardiac troponin; UDMI = Universal Definition of Myocardial Infarction.
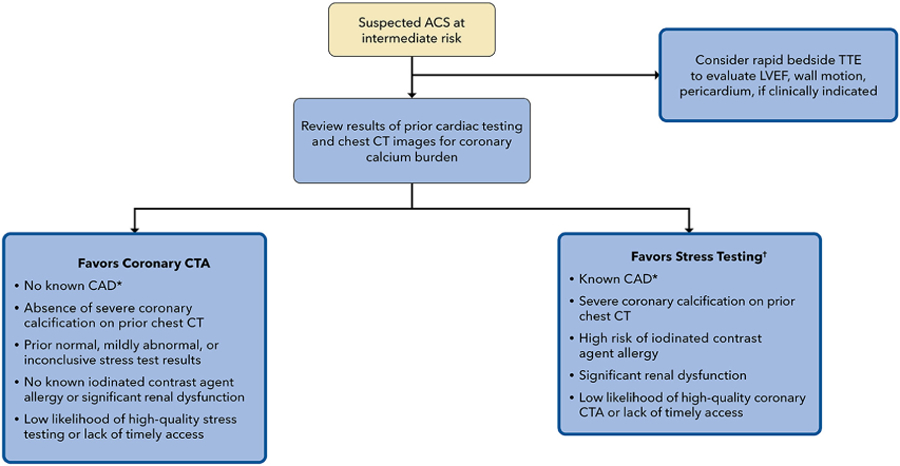
*Prior myocardial infarction, coronary revascularization, or stenosis >50% or extensive nonobstructive CAD on prior ICA/CTA. †Exercise ECG, stress CMR, stress echocardiography, stress perfusion imaging. ACS = acute coronary syndrome; CAD = coronary artery disease; CT = computed tomography; CTA = computed tomography angiography; ICA = internal carotid artery; LVEF = left ventricle ejection fraction; TTE = transthoracic echocardiogram.
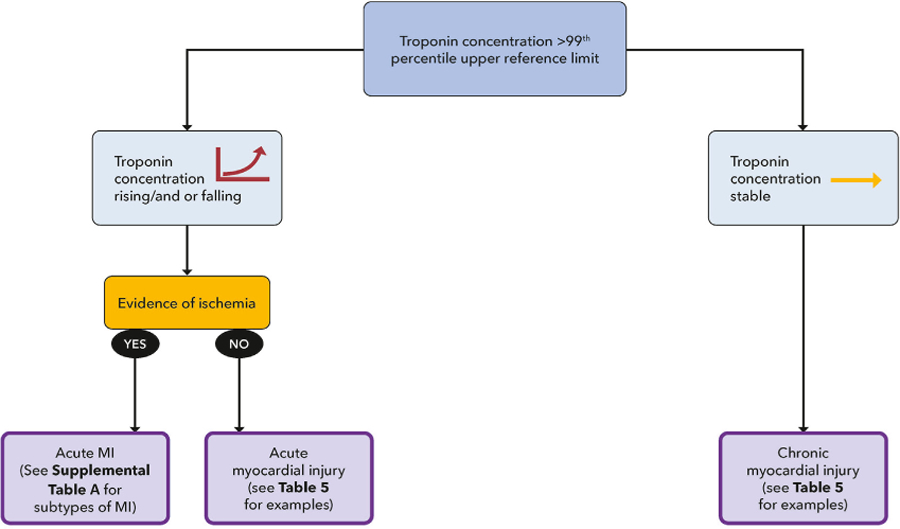
MI = myocardial infarction.
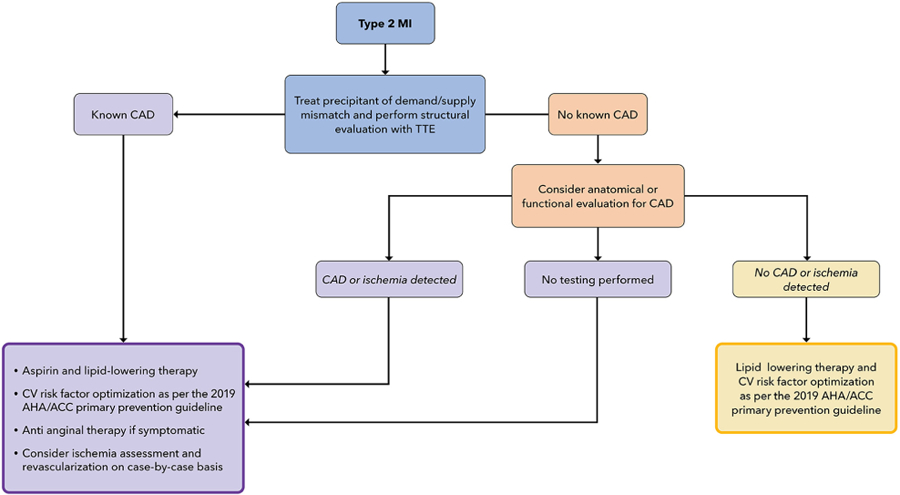
ACC = American College of Cardiology; AHA = American Heart Association; CAD = coronary artery disease; CV = cardiovascular; MI = myocardial infarction; TTE = transthoracic echocardiogram.
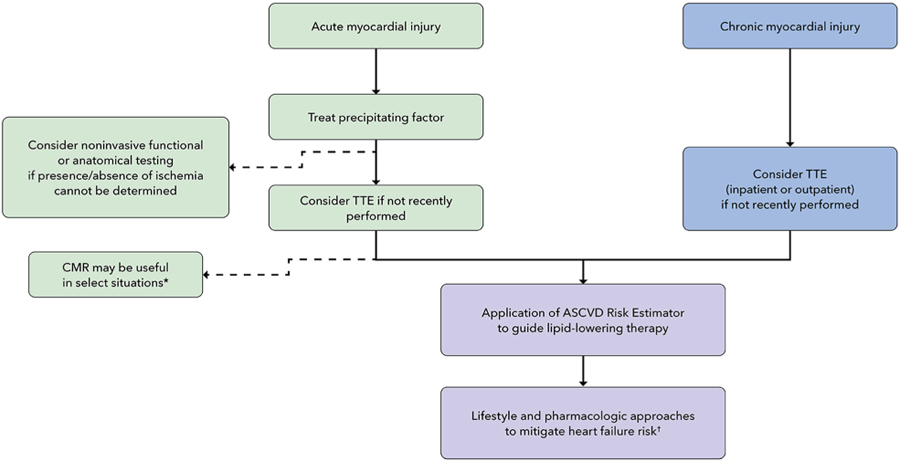
* Concern for myocarditis, hypertrophic cardiomyopathy, infiltrative cardiomyopathies. † Ensure blood pressure and diabetes are optimized; encourage increased physical activity and weight loss in overweight and obese individuals. ACC = American College of Cardiology; AHA = American Heart Association; ASCVD = atherosclerotic cardiovascular disease; CMR = cardiac magnetic resonance imaging; TTE = transthoracic echocardiogram.
References
-
- Januzzi JL Jr, Ahmad T, Binder LG, et al. 2019 methodology for creating expert consensus decision pathways: a report of the American College of Cardiology. J Am Coll Cardiol 2019;74:1138–1150. - PubMed
-
- Cairns C, Kang K, Santoc L. National Hospital Ambulatory Medical Care Survey: 2018 emergency department summary tables U.S. Department of Health and Human Services; 2018.
-
- Lindsell CJ, Anantharaman V, Diercks D, et al. The Internet Tracking Registry of Acute Coronary Syndromes (i*trACS): a multicenter registry of patients with suspicion of acute coronary syndromes reported using the standardized reporting guidelines for emergency department chest pain studies. Ann Emerg Med 2006;48:666–677, 677.e661–669. - PubMed
-
- Hsia RY, Hale Z, Tabas JA. A national study of the prevalence of life-threatening diagnoses in patients with chest pain. JAMA Intern Med 2016;176:1029–1032. - PubMed
-
- Gulati M, Levy PD, Mukherjee D, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the evaluation and diagnosis of chest pain: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2021;78:e187–e285. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
