

Characteristics Associated with Spirometry Guideline Adherence in VA Patients Hospitalized with Chronic Obstructive Pulmonary Disease
- PMID: 36241942
- PMCID: PMC9971396
- DOI: 10.1007/s11606-022-07826-5
Characteristics Associated with Spirometry Guideline Adherence in VA Patients Hospitalized with Chronic Obstructive Pulmonary Disease
Abstract
Background: The Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommends at least annual spirometry for patients with chronic obstructive pulmonary disease (COPD). Since spirometry acquisition is variable in clinical practice, identifying characteristics associated with annual spirometry may inform strategies to improve care for patients with COPD.
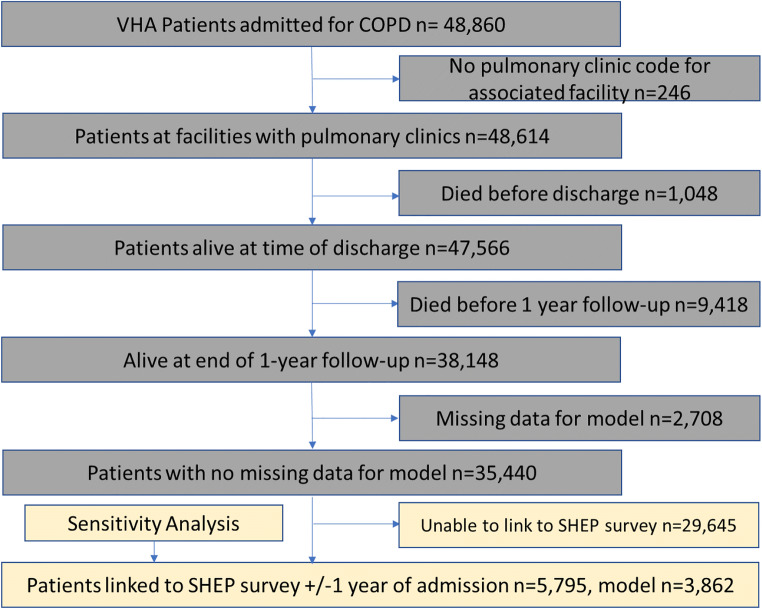
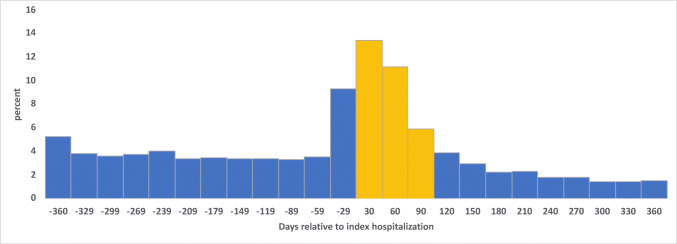
Methods: We included veterans hospitalized for COPD at Veterans Health Administration (VHA) facilities from 10/2012 to 09/2015. Our primary outcome was spirometry within 1 year of COPD hospitalization. Patient demographics, health factors, and comorbidities as well as practice and geographic variables were identified using Corporate Data Warehouse; provider characteristics were obtained from the Survey of Healthcare Experiences of Patients. We used logistic regression with a random intercept to account for potential clustering within facilities.
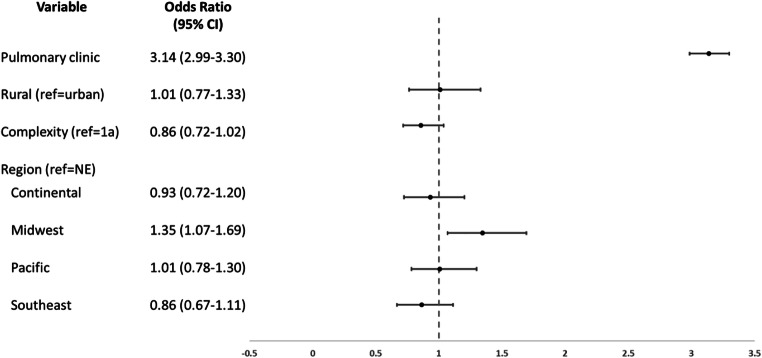
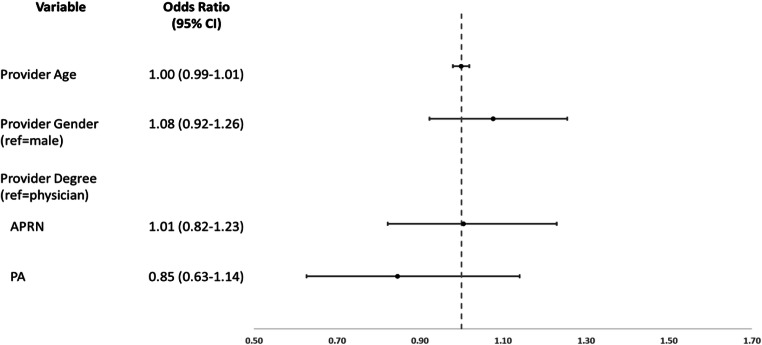
Results: Spirometry was completed 1 year before or after hospitalization for 20,683/38,148 (54.2%) veterans across 114 facilities. Patients with spirometry were younger, (mean=67.2 years (standard deviation (SD)=9.3) vs. 69.4 (10.3)), more likely non-white (21.3% vs. 19.7%), and more likely to have comorbidities (p<0.0001 for asthma, depression, and post-traumatic stress disorder). Pulmonary clinic visit was most strongly associated with spirometry (odds ratio (OR)=3.14 [95% confidence interval 2.99-3.30]). There was no association for facility complexity. In a secondary analysis including provider-level data (3862 patients), results were largely unchanged. There was no association between primary care provider age, gender, or type (physician vs. advanced practice registered nurse vs. physician assistant) and spirometry.
Conclusion: In a cohort of high-risk COPD patients, just over half completed spirometry within 1 year of hospitalization. Pulmonary clinic visit was most strongly associated with 1-year spirometry, though provider variables were not. Spirometry completion for high-risk COPD patients remains suboptimal and strategies to improve post-hospitalization care for patients not seen in pulmonary clinic should be developed to ensure guideline concordant care.
© 2022. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Diagnosing Chronic Obstructive Pulmonary Disease Among Afghanistan and Iraq Veterans: Veterans Affair's Concordance With Clinical Guidelines for Spirometry Administration.Mil Med. 2017 Sep;182(9):e1993-e2000. doi: 10.7205/MILMED-D-16-00332. Mil Med. 2017. PMID: 28885968 Free PMC article.
-
Drive Time and Receipt of Guideline-Recommended Screening, Diagnosis, and Treatment.JAMA Netw Open. 2022 Nov 1;5(11):e2240290. doi: 10.1001/jamanetworkopen.2022.40290. JAMA Netw Open. 2022. PMID: 36331503 Free PMC article.
-
Barriers to adherence to chronic obstructive pulmonary disease guidelines by primary care physicians.Int J Chron Obstruct Pulmon Dis. 2011;6:171-9. doi: 10.2147/COPD.S16396. Epub 2011 Feb 28. Int J Chron Obstruct Pulmon Dis. 2011. PMID: 21468169 Free PMC article.
-
Review: clinical inertia in the management of chronic obstructive pulmonary disease.COPD. 2012 Feb;9(1):73-80. doi: 10.3109/15412555.2011.631957. COPD. 2012. PMID: 22292599 Review.
-
Diagnostic and Therapeutic Gaps in Patients With Heart Failure and Chronic Obstructive Pulmonary Disease.JACC Heart Fail. 2019 Oct;7(10):823-833. doi: 10.1016/j.jchf.2019.05.009. Epub 2019 Sep 11. JACC Heart Fail. 2019. PMID: 31521680 Review.
References
-
- Akinbami L, Liu X. Chronic Obstructive Pulmonary Disease Among Adults Aged 18 and Over in the United States, 1998–2009. NCHS Data Brief. 2011. - PubMed
-
- VA/DoD Clinical Practice Guideline for the Mangement of Chronic Obstructive Pulmonary Disease. Department of Veterans Affiars, Department of Defense. 2014. https://www.healthquality.va.gov/guidelines/CD/copd/VADoDCOPDCPG2014.pdf. Accessed December 23, 2019.
-
- Finklestein J, Cha E. Association of Veteran status with COPD prevalence stratified by gender. Am J Respir Crit Care Med. 2013;187.
-
- Ramsey SD. Suboptimal medical therapy in COPD: exploring the causes and consequences. Chest. 2000;117:33S-7S. - PubMed
-
- Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2020 Report). 2020. https://goldcopd.org/wp-content/uploads/2019/12/GOLD-2020-FINAL-ver1.2-0.... Accessed December 23, 2019.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
