

Clinical evaluation of fenestration decompression combined with secondary curettage for ameloblastoma of the jaw: retrospective radiographic analysis
- PMID: 36242034
- PMCID: PMC9563122
- DOI: 10.1186/s12903-022-02474-x
Clinical evaluation of fenestration decompression combined with secondary curettage for ameloblastoma of the jaw: retrospective radiographic analysis
Abstract
Background: Ameloblastoma is a benign odontogenic epithelial tumor with local infiltration and a high recurrence rate that occurs most frequently in the jawbone. The aim of this study was to investigate the outcomes of fenestration decompression combined with secondary curettage (FDSC) in the surgical treatment of jaw ameloblastoma, and clarify the possibility of FDSC to become an appropriate therapeutic method for ameloblastoma with large lesion.
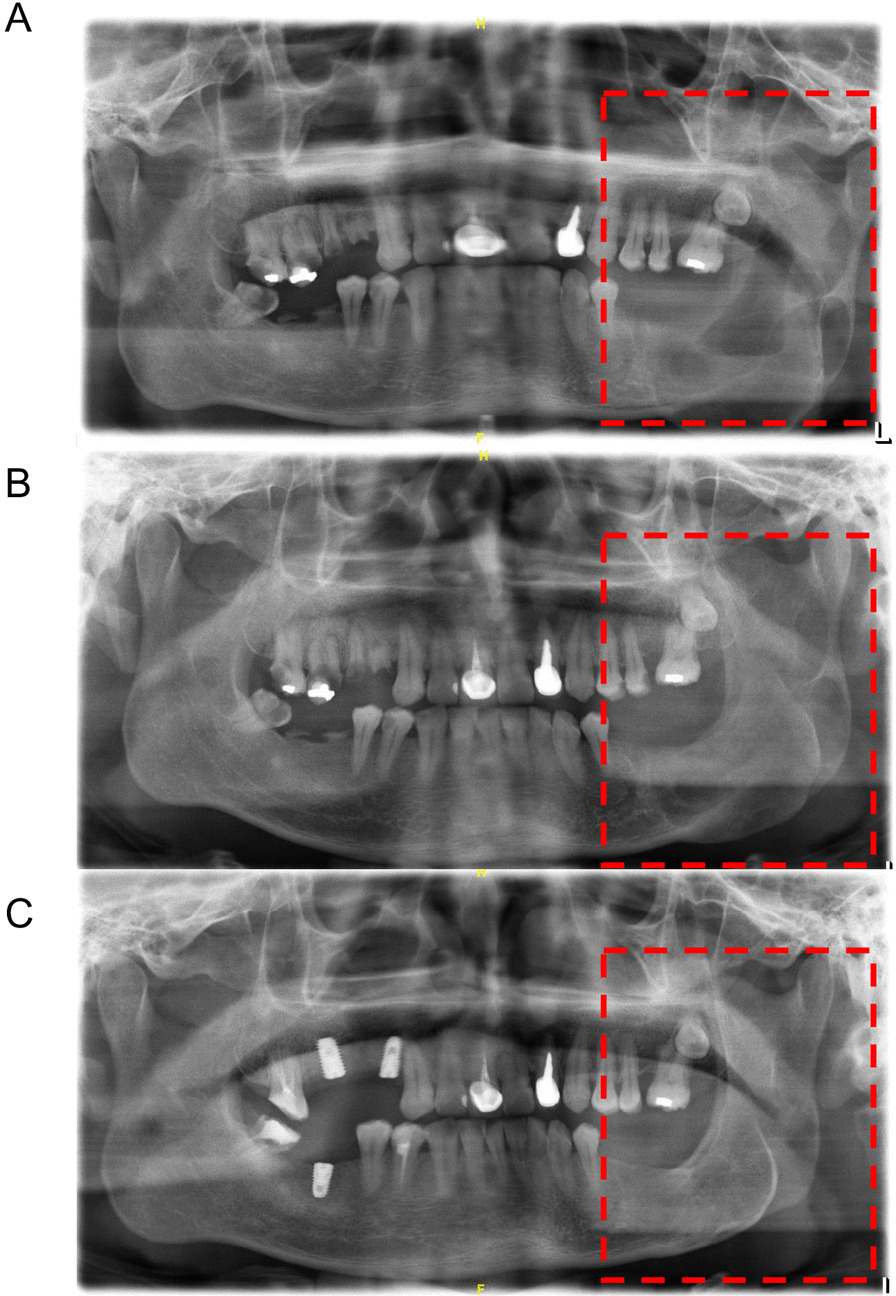
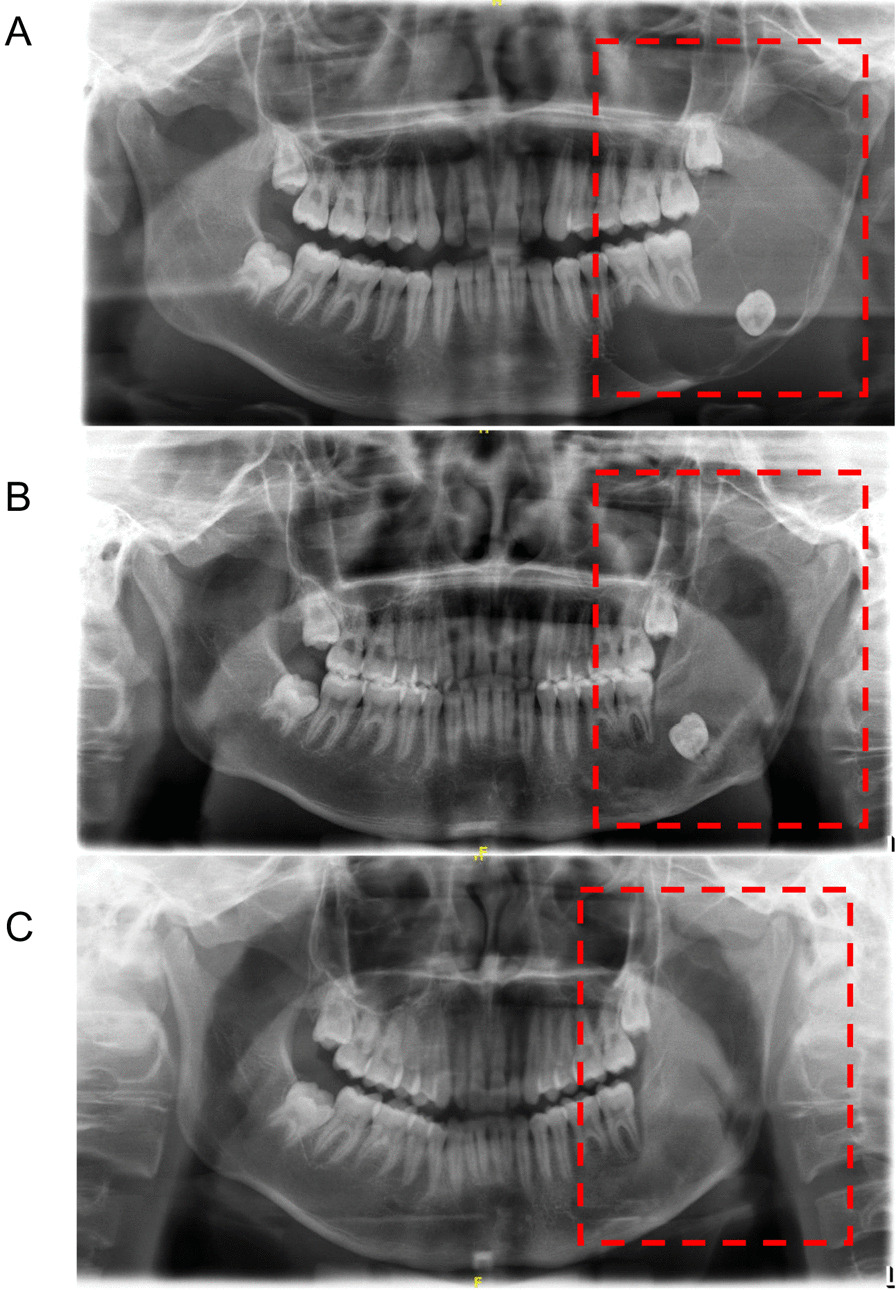
Methods: A retrospective analysis was carried out in 145 patients diagnosed with multicystic ameloblastoma (MA) and 88 patients with unicystic ameloblastoma (UA). These patients were divided into two groups based on the therapeutic regimen: the FDSC group and the local curettage (LC) group. Panoramic radiography was taken 2 years after curettage to evaluate the change in lesion area in each case, and the therapeutic effects of different treatment methods were further assessed by the chi square test.
Results: For MA, the effective rate of cystic cavity area reduction in the FDSC group (71.19%) was higher than that in the LC group (30.23%) (P < 0.001). For UA patients, the effective rate of lesion area reduction after FDSC was 93.02%, which was higher than that after LC (53.33%) (P < 0.001). Moreover, the recurrence rate of the FDSC group in the MA was 30.51%, which was significantly different from that of the LC group (P < 0.001). Regarding UA, the recurrence rates were 13.95% and 28.89%, after FDSC and LC, respectively, with no significant differences between the two groups (P > 0.05).
Conclusions: FDSC exhibits a much better curative effect than LC in both MA and UA, whereas the recurrence rate of these two therapeutic strategies did not significantly differ in UA. The above data demonstrated that FDSC may serve as a routine, safe, effective and appropriate surgical treatment plan for MA or UA patients with large lesions.
Keywords: Ameloblastoma; Curettage; Decompression; Recurrence; Retrospective study.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Curettage combined with decompression for the treatment of ameloblastoma in children: report of two cases.BMC Oral Health. 2024 Mar 22;24(1):378. doi: 10.1186/s12903-024-04126-8. BMC Oral Health. 2024. PMID: 38519948 Free PMC article.
-
Marsupialization of mandibular cystic ameloblastoma: Retrospective study of 7 years.Head Neck. 2018 Oct;40(10):2172-2180. doi: 10.1002/hed.25212. Epub 2018 May 13. Head Neck. 2018. PMID: 29756338
-
Conservative approach: using decompression procedure for management of a large unicystic ameloblastoma of the mandible.J Craniofac Surg. 2014 May;25(3):1012-4. doi: 10.1097/SCS.0000000000000716. J Craniofac Surg. 2014. PMID: 24699101
-
Conservative management is effective in unicystic ameloblastoma occurring from the neonatal period: A case report and a literature review.Oral Surg Oral Med Oral Pathol Oral Radiol. 2020 May;129(5):e234-e242. doi: 10.1016/j.oooo.2019.08.009. Epub 2019 Sep 6. Oral Surg Oral Med Oral Pathol Oral Radiol. 2020. PMID: 31562035 Review.
-
Potential role of active decompression and distraction sugosteogenesis for the management of ameloblastomas: Report of two cases and review of the literature.Oral Surg Oral Med Oral Pathol Oral Radiol. 2022 Aug;134(2):e29-e38. doi: 10.1016/j.oooo.2021.09.014. Epub 2021 Oct 4. Oral Surg Oral Med Oral Pathol Oral Radiol. 2022. PMID: 34972673 Review.
Cited by
-
Giant Mandibular Ameloblastoma with Rare Hypercalcemia: A Case Report and Literature Review.Medicina (Kaunas). 2023 Nov 6;59(11):1956. doi: 10.3390/medicina59111956. Medicina (Kaunas). 2023. PMID: 38004005 Free PMC article. Review.
-
A three-dimensional quantitative assessment on bony growth and symmetrical recovery of mandible after decompression for unicystic ameloblastoma.Sci Rep. 2024 Jul 5;14(1):15492. doi: 10.1038/s41598-024-66411-4. Sci Rep. 2024. PMID: 38969711 Free PMC article.
-
Curettage combined with decompression for the treatment of ameloblastoma in children: report of two cases.BMC Oral Health. 2024 Mar 22;24(1):378. doi: 10.1186/s12903-024-04126-8. BMC Oral Health. 2024. PMID: 38519948 Free PMC article.
References
-
- Oginni FO, Stoelinga PJ, Ajike SA, Obuekwe ON, Olokun BA, Adebola RA, Adeyemo WL, Fasola O, Adesina OA, Akinbami BO, et al. A prospective epidemiological study on odontogenic tumours in a black African population, with emphasis on the relative frequency of ameloblastoma. Int J Oral Maxillofac Surg. 2015;44(9):1099–1105. doi: 10.1016/j.ijom.2015.03.018. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
