

The burden of bacterial antimicrobial resistance in the WHO European region in 2019: a cross-country systematic analysis
- PMID: 36244350
- PMCID: PMC9630253
- DOI: 10.1016/S2468-2667(22)00225-0
The burden of bacterial antimicrobial resistance in the WHO European region in 2019: a cross-country systematic analysis
Abstract
Background: Antimicrobial resistance (AMR) represents one of the most crucial threats to public health and modern health care. Previous studies have identified challenges with estimating the magnitude of the problem and its downstream effect on human health and mortality. To our knowledge, this study presents the most comprehensive set of regional and country-level estimates of AMR burden in the WHO European region to date.
Methods: We estimated deaths and disability-adjusted life-years attributable to and associated with AMR for 23 bacterial pathogens and 88 pathogen-drug combinations for the WHO European region and its countries in 2019. Our methodological approach consisted of five broad components: the number of deaths in which infection had a role, the proportion of infectious deaths attributable to a given infectious syndrome, the proportion of infectious syndrome deaths attributable to a given pathogen, the percentage of a given pathogen resistant to an antimicrobial drug of interest, and the excess risk of mortality (or duration of an infection) associated with this resistance. These components were then used to estimate the disease burden by using two counterfactual scenarios: deaths attributable to AMR (considering an alternative scenario where infections with resistant pathogens are replaced with susceptible ones) and deaths associated with AMR (considering an alternative scenario where drug-resistant infections would not occur at all). Data were solicited from a wide array of international stakeholders; these included research hospitals, surveillance networks, and infection databases maintained by private laboratories and medical technology companies. We generated 95% uncertainty intervals (UIs) for final estimates as the 25th and 975th ordered values across 1000 posterior draws, and models were cross-validated for out-of-sample predictive validity.
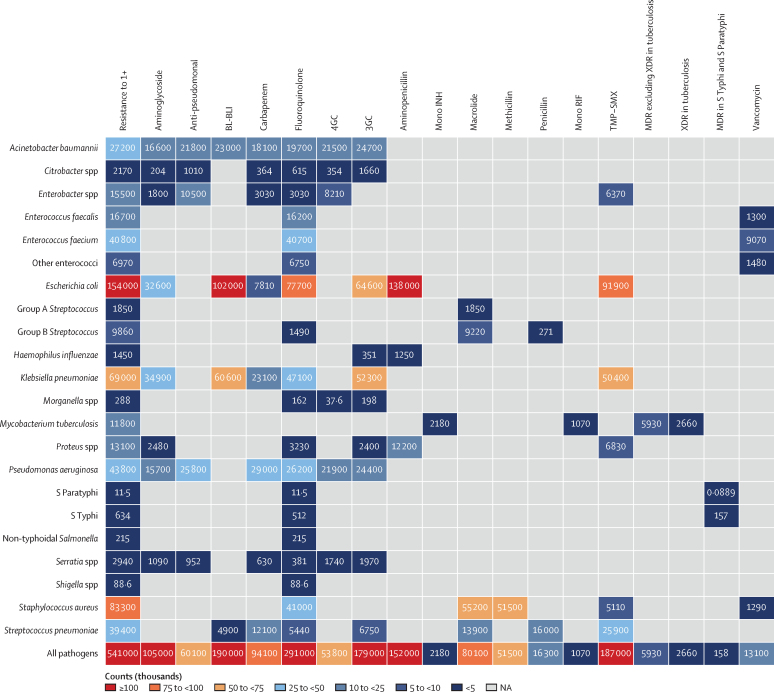
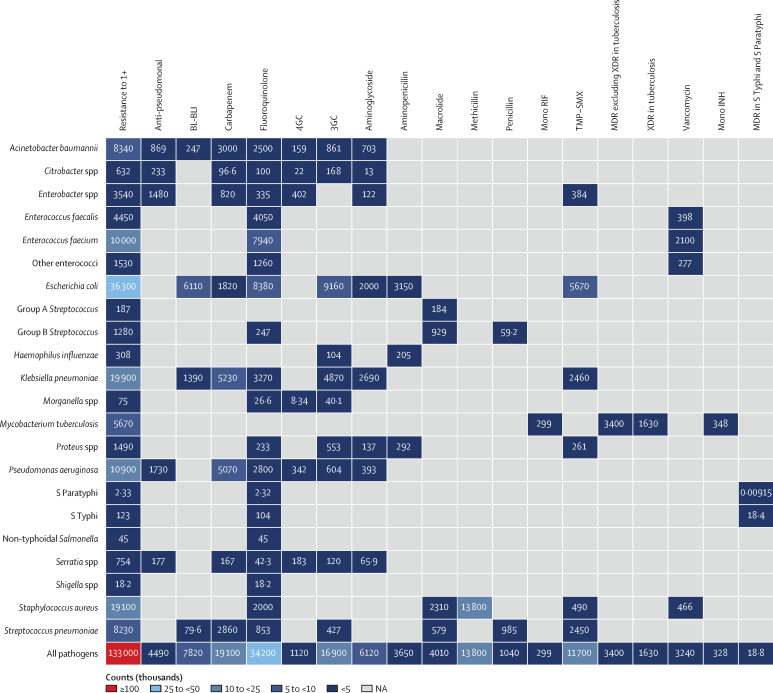
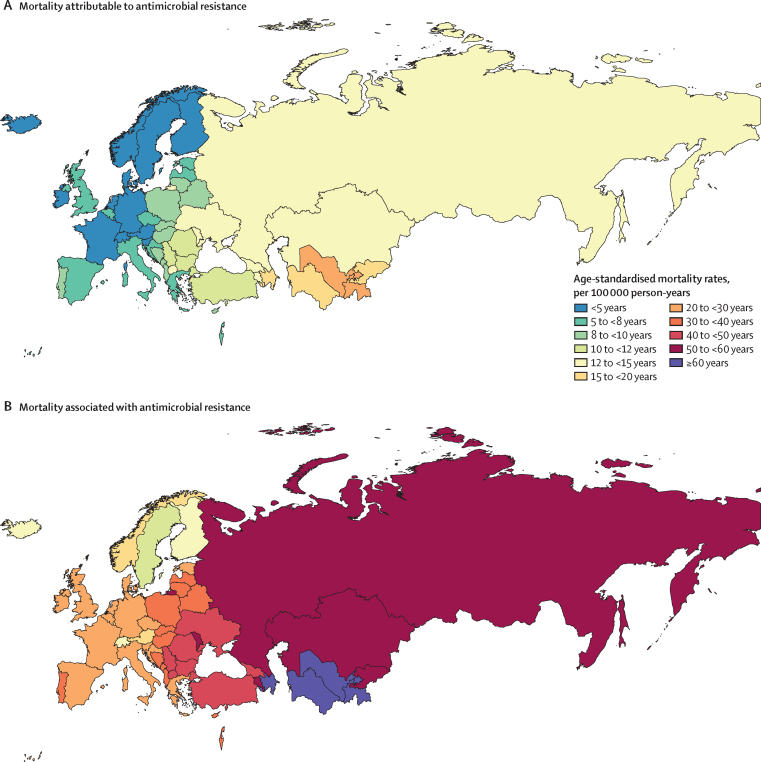
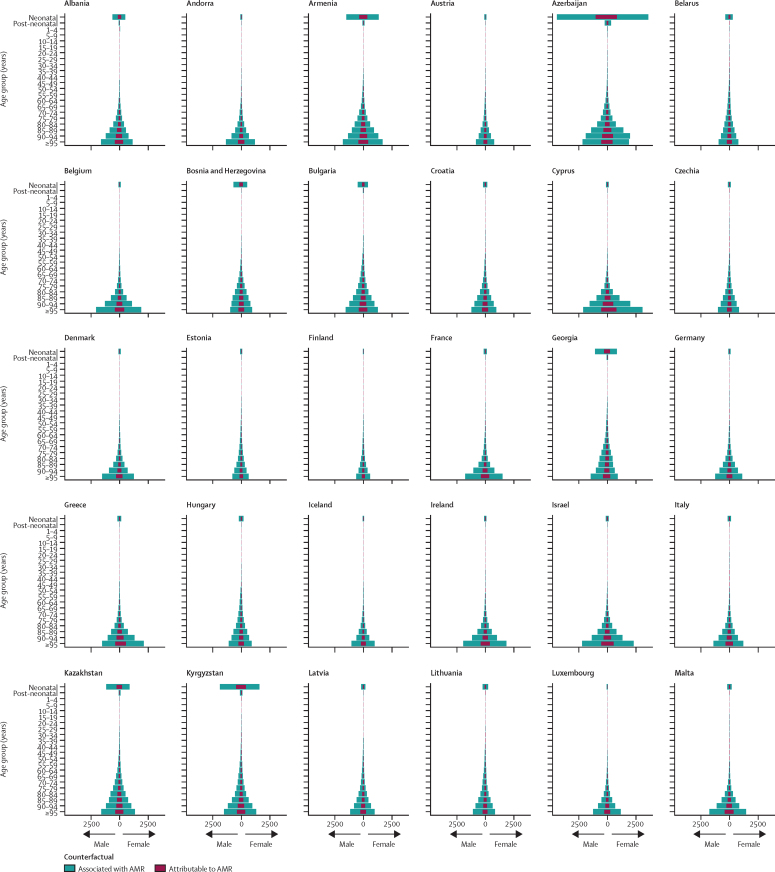
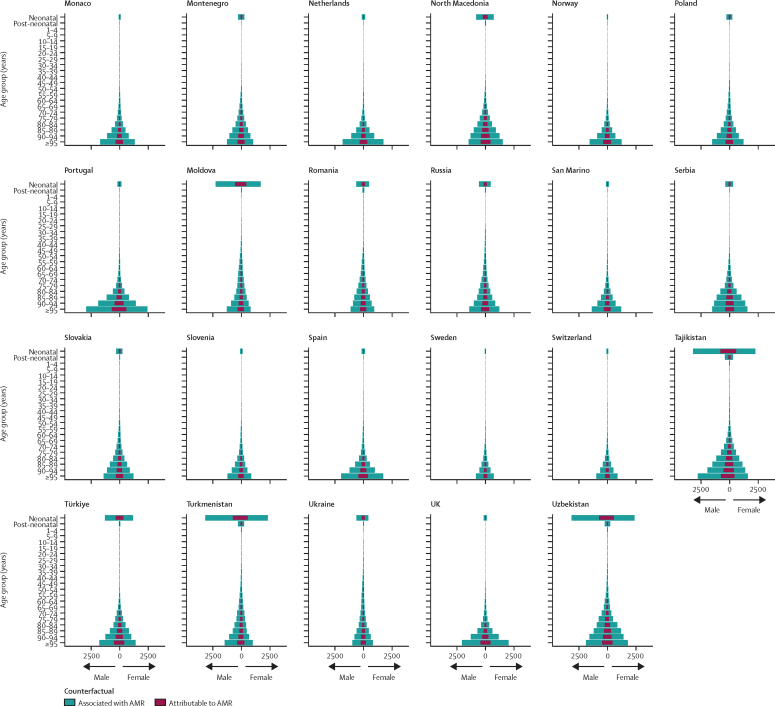
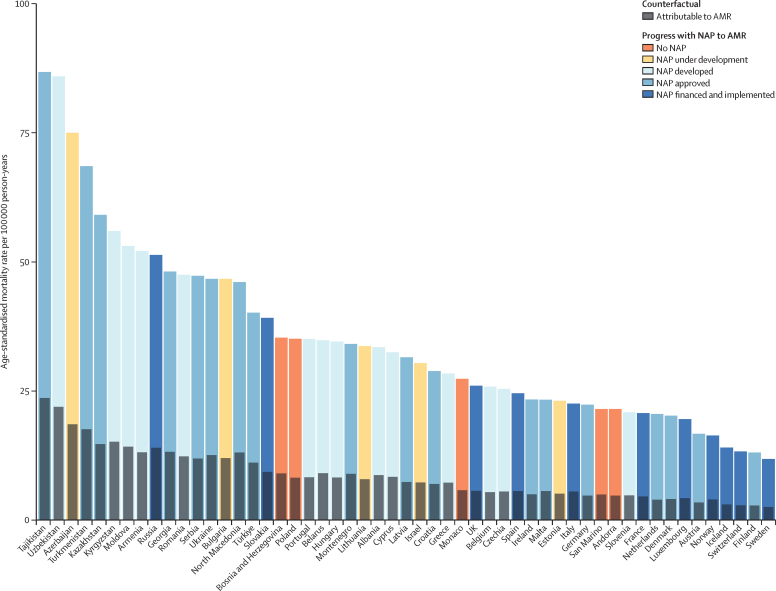
Findings: We estimated 541 000 deaths (95% UI 370 000-763 000) associated with bacterial AMR and 133 000 deaths (90 100-188 000) attributable to bacterial AMR in the whole WHO European region in 2019. The largest fatal burden of AMR in the region came from bloodstream infections, with 195 000 deaths (104 000-333 000) associated with resistance, followed by intra-abdominal infections (127 000 deaths [81 900-185 000]) and respiratory infections (120 000 deaths [94 500-154 000]). Seven leading pathogens were responsible for about 457 000 deaths associated with resistance in 53 countries of this region; these pathogens were, in descending order of mortality, Escherichia coli, Staphylococcus aureus, Klebsiella pneumoniae, Pseudomonas aeruginosa, Enterococcus faecium, Streptococcus pneumoniae, and Acinetobacter baumannii. Methicillin-resistant S aureus was shown to be the leading pathogen-drug combination in 27 countries for deaths attributable to AMR, while aminopenicillin-resistant E coli predominated in 47 countries for deaths associated with AMR.
Interpretation: The high levels of resistance for several important bacterial pathogens and pathogen-drug combinations, together with the high mortality rates associated with these pathogens, show that AMR is a serious threat to public health in the WHO European region. Our regional and cross-country analyses open the door for strategies that can be tailored to leading pathogen-drug combinations and the available resources in a specific location. These results underscore that the most effective way to tackle AMR in this region will require targeted efforts and investments in conjunction with continuous outcome-based research endeavours.
Funding: Bill & Melinda Gates Foundation, Wellcome Trust, and Department of Health and Social Care using UK aid funding managed by the Fleming Fund.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests RA reports consulting fees from AbbVie; and payment or honoraria for lectures, presentations, speaker's bureaus, manuscript writing, or educational events from AbbVie, B Braun, Sandoz, and Laropharm, all outside the submitted work. CH and AP report grants from the Romanian National Authority for Scientific Research and Innovation, CNDS-UEFISCDI, for project number PN-III-P4-ID-PCCF-2016-0084 and project number PN-III-P2-2.1-SOL-2020-2-0351, outside the submitted work. CH also reports grants from the Romanian Ministry of Research Innovation and Digitalization MCID for project number ID-585-CTR-42-PFE-2021, outside the submitted work. A-FAM reports grants or contracts from MilkSafe, research co-financed by the EU European Regional Development Fund and Greek national funds through the operational programme Competitiveness, Entrepreneurship and Innovation, under the call RESEARCH–CREATE–INNOVATE (T2EDK-02222), as well as from ELIDEK (Hellenic Foundation for Research and Innovation, MIMS-860); stocks in a family winery; and other financial or non-financial interests in the BGI Group as a scientific officer, all outside of the submitted work. BS reports grants or contracts from the Fleming Fund; and leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid, with the GBD Scientific Council and WHO RGHS, all outside the submitted work. AS reports support for the present manuscript from the Bill & Melinda Gates Foundation as payment to their institution, and paid participation on a Scientific Advisory Board for Vivli, outside the submitted work. All other authors declare no competing interests.
Figures
Comment in
-
Estimating antimicrobial resistance burden in Europe-what are the next steps?Lancet Public Health. 2022 Nov;7(11):e886-e887. doi: 10.1016/S2468-2667(22)00250-X. Epub 2022 Oct 14. Lancet Public Health. 2022. PMID: 36244349 No abstract available.
References
-
- O'Neill J. The Review on Antimicrobial Resistance; London: 2016. Tackling drug-resistant infections globally: final report and recommendations.
-
- National Office for Animal Health NOAH response to final O Neill AMR review report. 2016. https://www.noah.co.uk/wp-content/uploads/2016/07/FINAL-NOAH-response-to...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
