

Sleep Arousal-Related Ventricular Repolarization Lability Is Associated With Cardiovascular Mortality in Older Community-Dwelling Men
- PMID: 36244405
- PMCID: PMC9899642
- DOI: 10.1016/j.chest.2022.09.043
Sleep Arousal-Related Ventricular Repolarization Lability Is Associated With Cardiovascular Mortality in Older Community-Dwelling Men
Abstract
Background: Sleep is fragmented by brief arousals, and excessive arousal burden has been linked to increased cardiovascular (CV) risk, but mechanisms are poorly understood.
Research question: Do arousals trigger cardiac ventricular repolarization lability that may predispose people to long-term cardiovascular mortality?
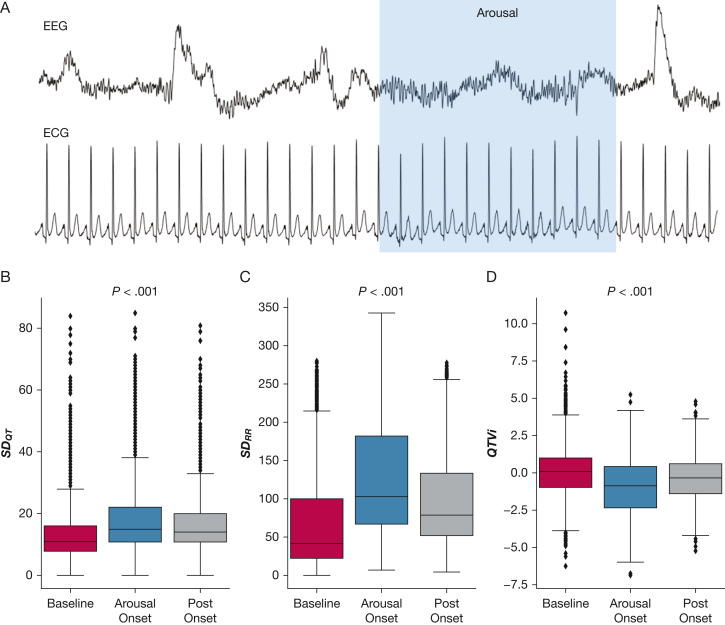
Study design and methods: This study analyzed 407,541 arousals in the overnight polysomnograms of 2,558 older men in the Osteoporotic Fractures in Men sleep study. QT and RR intervals were measured beat-to-beat starting 15 s prior to arousal onset until 15 s past onset. Ventricular repolarization lability was quantified by using the QT variability index (QTVi).
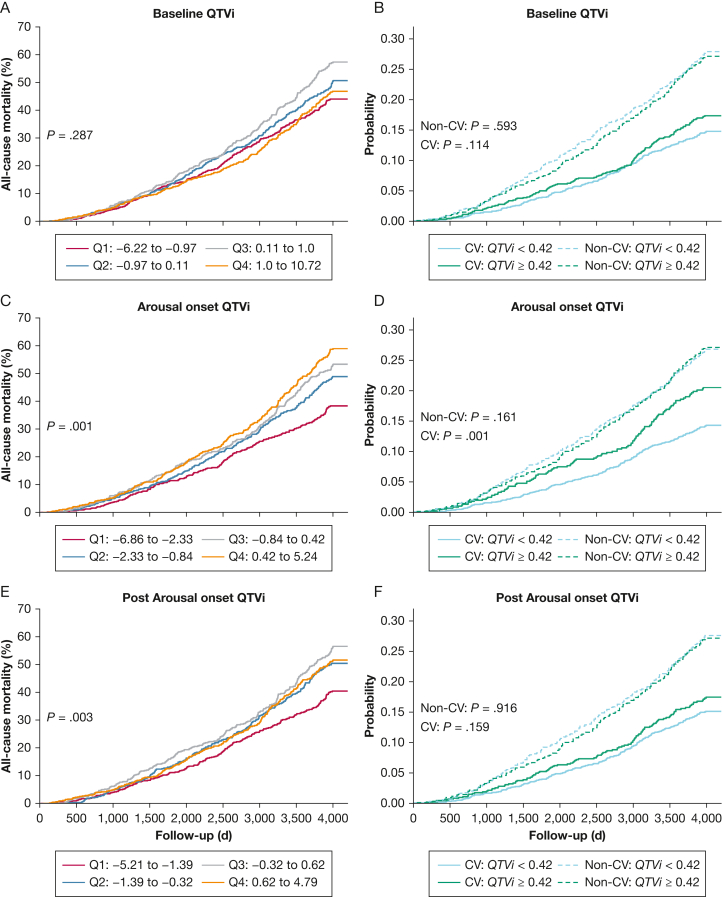
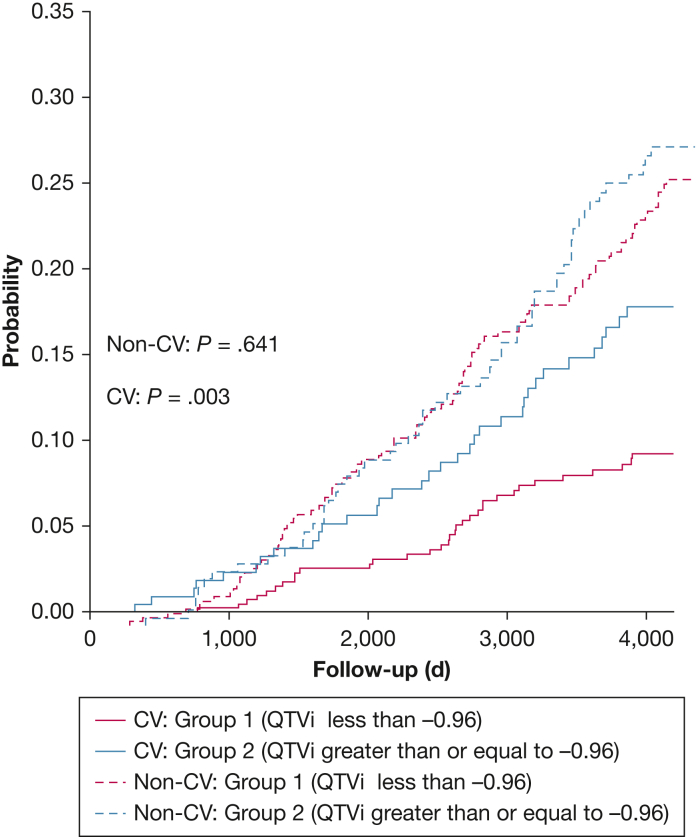
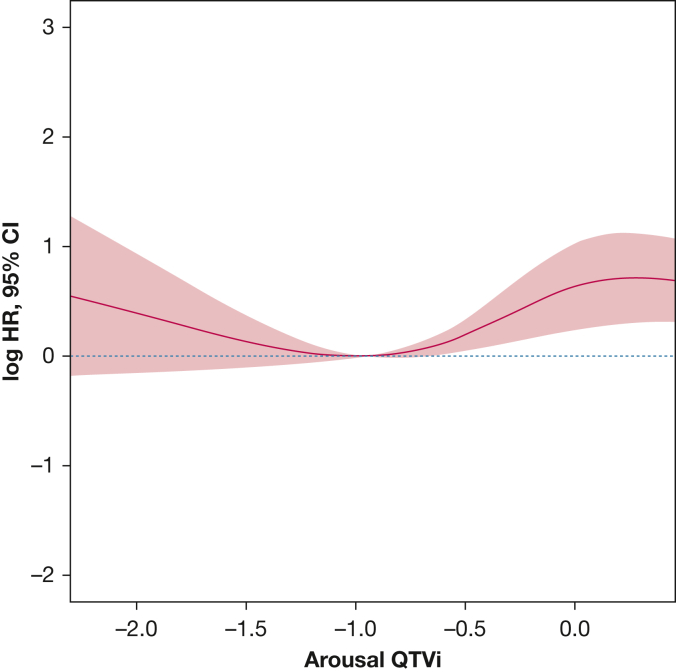
Results: During 10.1 ± 2.5 years of follow-up, 1,000 men died of any cause, including 348 CV deaths. During arousals, QT and RR variability increased on average by 5 and 55 ms, respectively, resulting in a paradoxical transient decrease in QTVi from 0.07 ± 1.68 to -1.00 ± 1.68. Multivariable Cox proportional hazards analysis adjusted for age, BMI, cardiovascular and respiratory risk factors, sleep-disordered breathing and arousal, diabetes, and Parkinson disease indicated that excessive QTVi during arousal was independently associated with all-cause and CV mortality (all-cause hazard ratio, 1.20 [95% CI, 1.04-1.38; P = .012]; CV hazard ratio, 1.29 [95% CI, 1.01 -1.65; P = .043]).
Interpretation: Arousals affect ventricular repolarization. A disproportionate increase in QT variability during arousal is associated with an increased all-cause and CV mortality and may reflect ventricular repolarization maladaptation to the arousal stimulus. Whether arousal-related QTVi can be used for more tailored risk stratification warrants further study, including evaluating whether arousal suppression attenuates ventricular repolarization lability and reduces subsequent mortality.
Clinical trial registration: ClinicalTrials.gov; No.: NCT00070681; URL: www.
Clinicaltrials: gov.
Keywords: QT variability index; all-cause mortality; cardiovascular mortality; sleep apnea; sleep arousal; ventricular repolarization.
Copyright © 2022 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Beat-to-beat cardiac repolarization lability increases during hypoxemia and arousals in obstructive sleep apnea patients.Am J Physiol Heart Circ Physiol. 2024 May 1;326(5):H1094-H1104. doi: 10.1152/ajpheart.00760.2023. Epub 2024 Mar 1. Am J Physiol Heart Circ Physiol. 2024. PMID: 38426864 Free PMC article.
-
Sleep-disordered breathing destabilizes ventricular repolarization: Cross-sectional, longitudinal, and experimental evidence.Heart Rhythm. 2025 Mar;22(3):808-816. doi: 10.1016/j.hrthm.2024.08.054. Epub 2024 Aug 28. Heart Rhythm. 2025. PMID: 39214391
-
HIV Infection Is Associated With Variability in Ventricular Repolarization: The Multicenter AIDS Cohort Study (MACS).Circulation. 2020 Jan 21;141(3):176-187. doi: 10.1161/CIRCULATIONAHA.119.043042. Epub 2019 Nov 11. Circulation. 2020. PMID: 31707799 Free PMC article. Clinical Trial.
-
QT Variability Index.Prog Cardiovasc Dis. 2013 Sep-Oct;56(2):186-94. doi: 10.1016/j.pcad.2013.07.004. Epub 2013 Oct 4. Prog Cardiovasc Dis. 2013. PMID: 24215750 Review.
-
[Sleep apnea syndromes and cardiovascular disease].Bull Acad Natl Med. 2005 Mar;189(3):445-59; discussion 460-4. Bull Acad Natl Med. 2005. PMID: 16149210 Review. French.
Cited by
-
Sleep-Disordered Breathing Destabilizes Ventricular Repolarization.medRxiv [Preprint]. 2024 Apr 12:2023.02.10.23285789. doi: 10.1101/2023.02.10.23285789. medRxiv. 2024. Update in: Heart Rhythm. 2025 Mar;22(3):808-816. doi: 10.1016/j.hrthm.2024.08.054. PMID: 36824787 Free PMC article. Updated. Preprint.
-
Clinical characteristics and outcomes of positional obstructive sleep apnea: the sleep heart health study.Eur Arch Otorhinolaryngol. 2025 Aug;282(8):4291-4298. doi: 10.1007/s00405-025-09409-6. Epub 2025 Apr 25. Eur Arch Otorhinolaryngol. 2025. PMID: 40281320
-
Beat-to-beat cardiac repolarization lability increases during hypoxemia and arousals in obstructive sleep apnea patients.Am J Physiol Heart Circ Physiol. 2024 May 1;326(5):H1094-H1104. doi: 10.1152/ajpheart.00760.2023. Epub 2024 Mar 1. Am J Physiol Heart Circ Physiol. 2024. PMID: 38426864 Free PMC article.
-
Arousal burden is highest in supine sleeping position and during light sleep.J Clin Sleep Med. 2025 Feb 1;21(2):337-344. doi: 10.5664/jcsm.11398. J Clin Sleep Med. 2025. PMID: 39364956
-
Hypoxaemic load in sleep apnoea is associated with acute changes in T-wave amplitude.ERJ Open Res. 2024 Oct 28;10(5):00341-2024. doi: 10.1183/23120541.00341-2024. eCollection 2024 Sep. ERJ Open Res. 2024. PMID: 39469266 Free PMC article.
References
-
- Iber C., Ancoli-Israel A., Chesson A., Quan S.F. American Academy of Sleep Medicine; 2007. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications.
-
- Cowie M.R., Linz D., Redline S., Somers V.K., Simonds A.K. Sleep disordered breathing and cardiovascular disease: JACC State-of-the-Art Review. J Am Coll Cardiol. 2021;78(6):608–624. - PubMed
-
- Floras J.S. Sympathetic nervous system in patients with sleep related breathing disorders. Cur Hypertension Rev. 2016;12(1):18–26. - PubMed
-
- Linz D., Baumert M., Catcheside P., et al. Assessment and interpretation of sleep disordered breathing severity in cardiology: clinical implications and perspectives. Int J Cardiol. 2018;271:281–288. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- R01 HL070848/HL/NHLBI NIH HHS/United States
- R01 HL071194/HL/NHLBI NIH HHS/United States
- R01 HL070847/HL/NHLBI NIH HHS/United States
- U01 AG042145/AG/NIA NIH HHS/United States
- U01 AG042168/AG/NIA NIH HHS/United States
- R01 HL070841/HL/NHLBI NIH HHS/United States
- R01 HL070839/HL/NHLBI NIH HHS/United States
- U01 AG027810/AG/NIA NIH HHS/United States
- U01 AG042139/AG/NIA NIH HHS/United States
- U01 AR066160/AR/NIAMS NIH HHS/United States
- R01 HL070842/HL/NHLBI NIH HHS/United States
- R01 AG066671/AG/NIA NIH HHS/United States
- U01 AG042124/AG/NIA NIH HHS/United States
- U01 AG042140/AG/NIA NIH HHS/United States
- R01 HL070838/HL/NHLBI NIH HHS/United States
- R01 HL070837/HL/NHLBI NIH HHS/United States
- U01 AG042143/AG/NIA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
