

Heterogeneity of Stroke in Patients with Systemic Lupus Erythematosus
- PMID: 36244734
- PMCID: PMC9646340
- DOI: 10.2169/internalmedicine.9228-21
Heterogeneity of Stroke in Patients with Systemic Lupus Erythematosus
Abstract
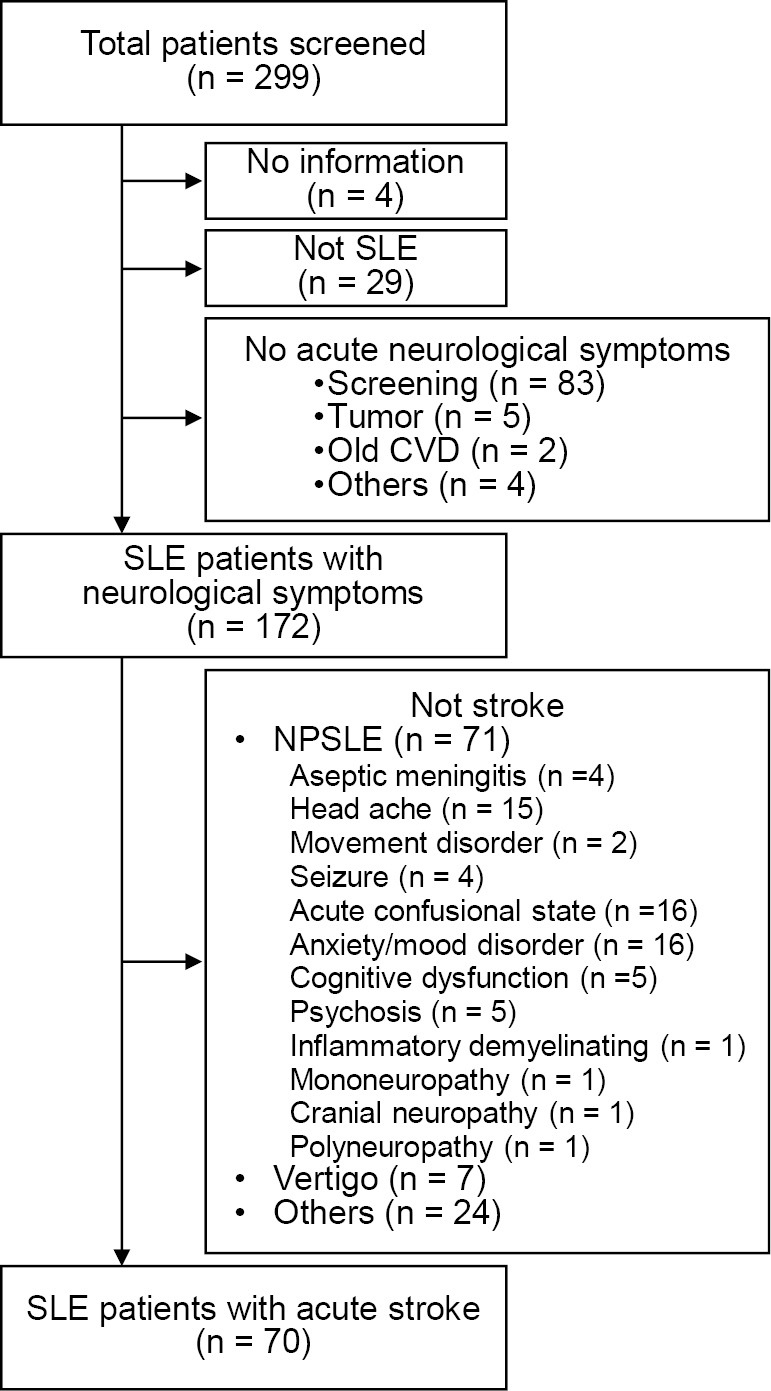
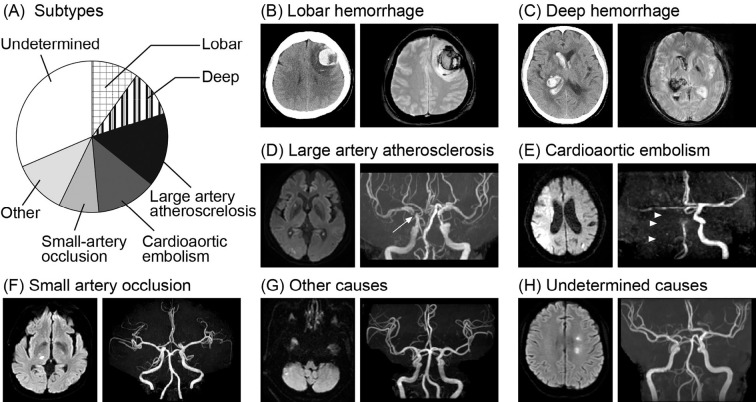
Objective The underlying pathophysiology varies according to stroke subtype. However, stroke heterogeneity among patients with systemic lupus erythematosus (SLE) remains unstudied. We hypothesized that the contribution of SLE to stroke might vary according to its subtype and investigated the associations of SLE and various stroke subtypes. Methods Diagnostic codes and electronic medical records were used to identify 70 patients with SLE who developed acute cerebral infarction or intracerebral hemorrhaging at four tertiary referral hospitals between 2008 and 2018. Intracerebral hemorrhaging was classified as lobar or deep, while cerebral infarction was classified according to the SSS-TOAST criteria. Physician notes were used to identify SLE activity, and their prevalences were compared among stroke subtypes. Outcomes were collected from the patients' medical records. Results The most common stroke subtype in patients with SLE was that of undetermined causes (31%), followed by small artery occlusion (16%), cardioaortic embolism (13%), other causes (11%), lobar hemorrhaging (10%), deep hemorrhaging (10%), and large artery atherosclerosis (9%). Stroke onset occurred during a period of high SLE activity in 21 patients (30%). The proportion of patients with high SLE activity varied according to stroke subtype (p=0.039) and was highest for cerebral infarction with undetermined causes. Stroke recurrence or death was observed in 40% of patients within 5 years after the initial stroke onset. Conclusion The contributions of SLE to stroke varied significantly according to the stroke subtype. Given the unfavorable prognosis, close stroke subtype-specific observation by rheumatologists and stroke specialists is recommended after stroke events.
Keywords: antiphospholipid syndrome; cerebrovascular disease; lupus; prognosis; stroke; thrombosis.
Conflict of interest statement
Figures



References
-
- Bertsias GK, Boumpas DT. Pathogenesis, diagnosis and management of neuropsychiatric SLE manifestations. Nature Rev Rheumatol 6: 358-367, 2010. - PubMed
-
- Hanly JG, Su L, Farewell V, McCurdy G, Fougere L, Thompson K. Prospective study of neuropsychiatric events in systemic lupus erythematosus. J Rheumatol 36: 1449-1459, 2009. - PubMed
-
- Mok CC, To CH, Mak A. Neuropsychiatric damage in Southern Chinese patients with systemic lupus erythematosus. Medicine 85: 221-228, 2006. - PubMed
-
- Zhou HQ, Zhang FC, Tian XP, et al. . Clinical features and outcome of neuropsychiatric lupus in Chinese: analysis of 240 hospitalized patients. Lupus 17: 93-99, 2008. - PubMed