

An Integrative Multi-Omics Analysis Based on Nomogram for Predicting Prostate Cancer Bone Metastasis Incidence
- PMID: 36245556
- PMCID: PMC9537037
- DOI: 10.1155/2022/8213723
An Integrative Multi-Omics Analysis Based on Nomogram for Predicting Prostate Cancer Bone Metastasis Incidence
Abstract
Background: The most common site of prostate cancer metastasis is bone tissue with many recent studies having conducted genomic and clinical research regarding bone metastatic prostate cancer. However, further work is needed to better define those patients that are at an elevated risk of such metastasis.
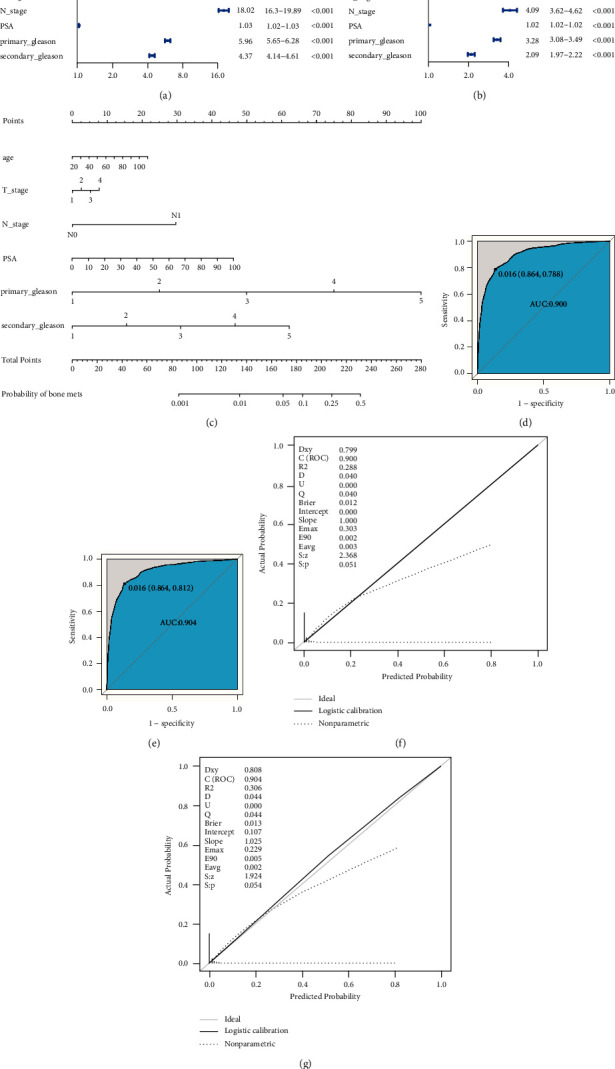
Methods: SEER and TCGA databases were searched to develop a nomogram for predicting prostate cancer bone metastasis.
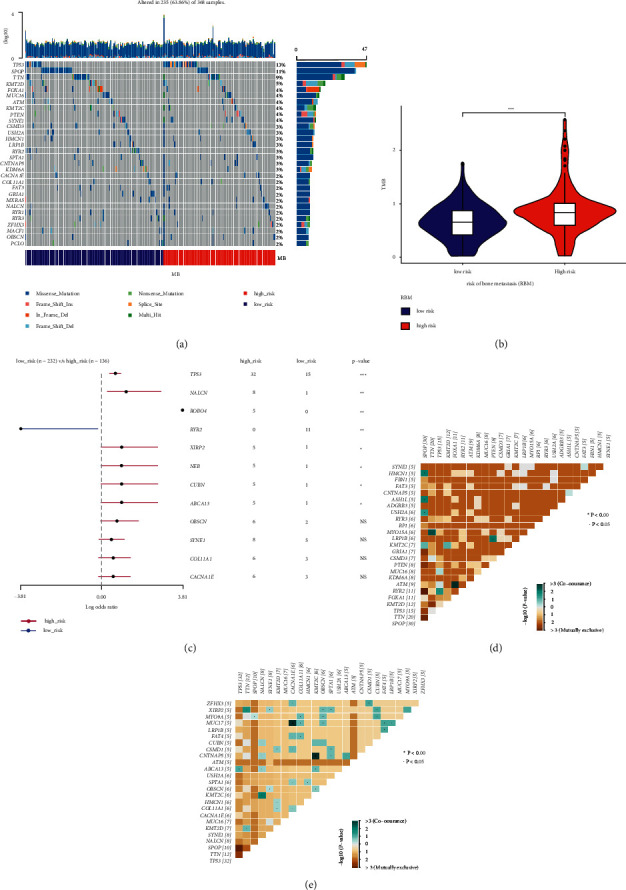
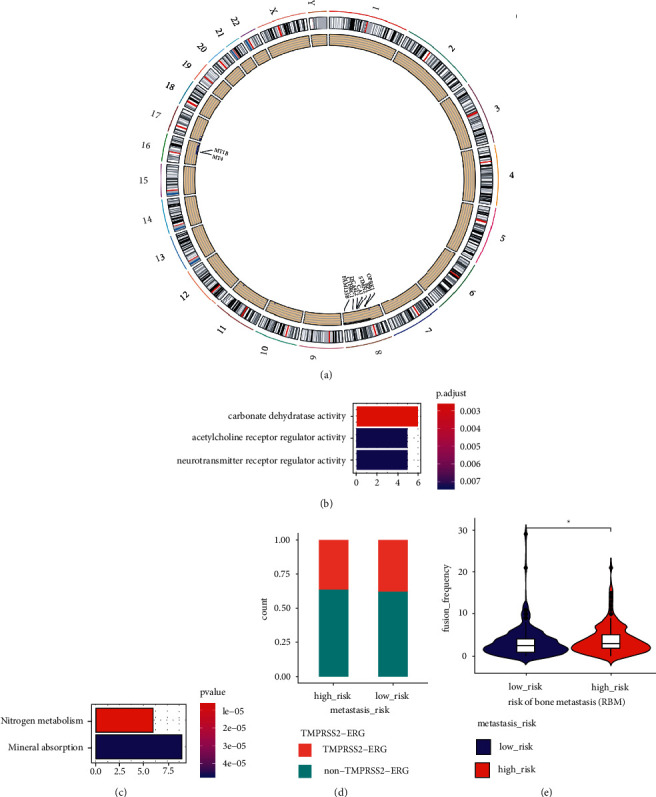
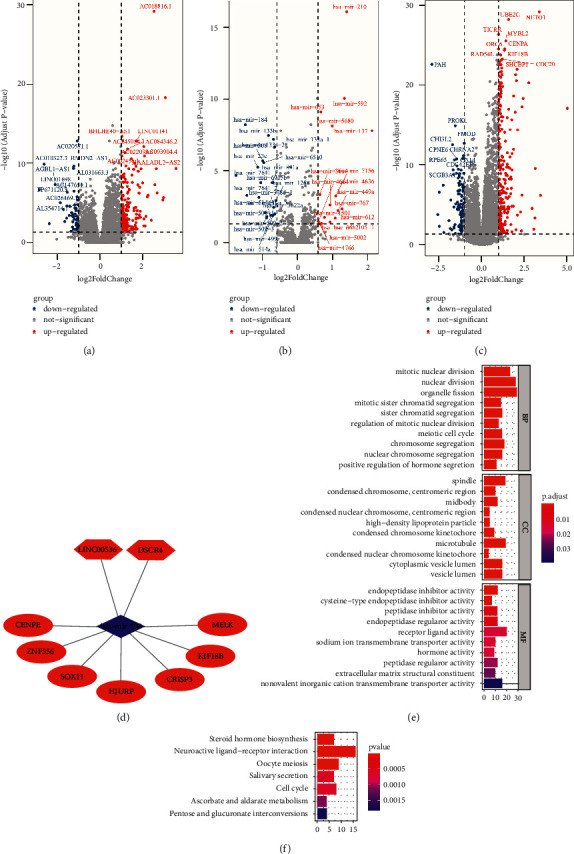
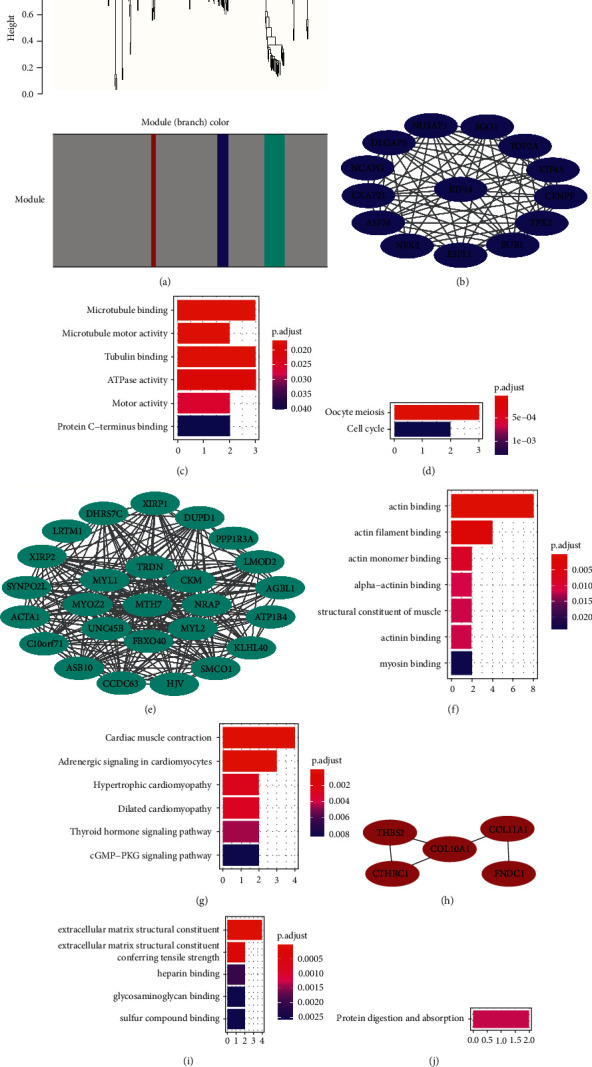
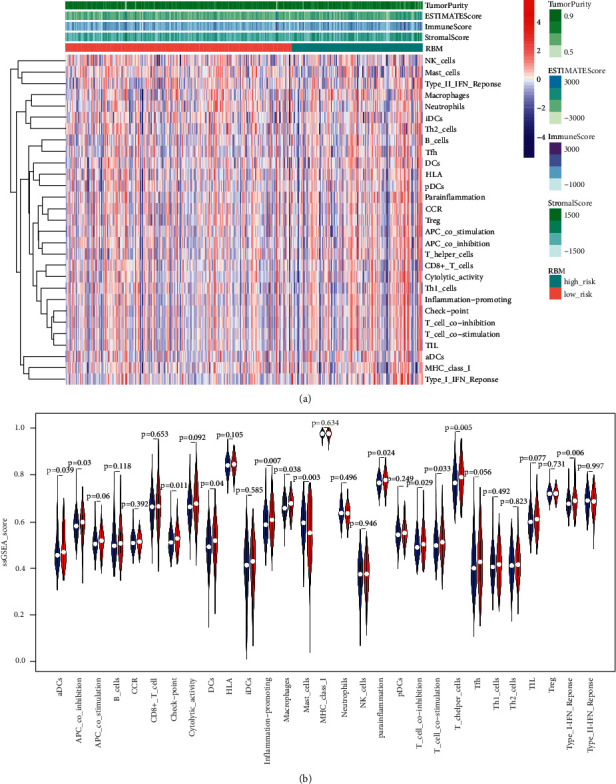
Results: Herein, we leveraged the Surveillance, Epidemiology, and End Results (SEER) database to construct a predictive nomogram capable of readily and accurately predicted the odds of bone metastasis in prostate cancer patients. This nomogram was utilized to assign patients with prostate cancer included in The Cancer Genome Atlas (TCGA) to cohorts at a high or low risk of bone metastasis (HRBM and LRBM, respectively). Comparisons of these LRBM and HRBM cohorts revealed marked differences in mutational landscapes between these patient cohorts, with increased frequencies of gene fusions, somatic copy number variations (CNVs), and single nucleotide variations (SNVs), particularly in the P53 gene, being evident in the HRBM cohort. We additionally identified lncRNAs, miRNAs, and mRNAs that were differentially expressed between these two patient cohorts and used them to construct a competing endogenous RNA (ceRNA) network. Moreover, three weighted gene co-expression network analysis (WGCNA) modules were constructed from the results of these analyses, with KIF14, MYH7, and COL10A1 being identified as hub genes within these modules. We further found immune response activity levels in the HRBM cohort to be elevated relative to that in the LRBM cohort, with single sample gene enrichment analysis (ssGSEA) scores for the immune checkpoint signature being increased in HRBM patient samples relative to those from LRBM patients.
Conclusion: We successfully developed a nomogram capable of readily detecting patients with prostate cancer at an elevated risk of bone metastasis.
Copyright © 2022 Jun Zhao et al.
Conflict of interest statement
The authors state that there are no conflicts of interest to declare.
Figures
Similar articles
-
Identification of HCG18 and MCM3AP-AS1 That Associate With Bone Metastasis, Poor Prognosis and Increased Abundance of M2 Macrophage Infiltration in Prostate Cancer.Technol Cancer Res Treat. 2021 Jan-Dec;20:1533033821990064. doi: 10.1177/1533033821990064. Technol Cancer Res Treat. 2021. PMID: 33596783 Free PMC article.
-
Construction of a ceRNA network and a genomic-clinicopathologic nomogram to predict survival for HBV-related HCC.Hum Cell. 2021 Nov;34(6):1830-1842. doi: 10.1007/s13577-021-00607-y. Epub 2021 Sep 6. Hum Cell. 2021. PMID: 34487338
-
Excavating novel diagnostic and prognostic long non-coding RNAs (lncRNAs) for head and neck squamous cell carcinoma: an integrated bioinformatics analysis of competing endogenous RNAs (ceRNAs) and gene co-expression networks.Bioengineered. 2021 Dec;12(2):12821-12838. doi: 10.1080/21655979.2021.2003925. Bioengineered. 2021. PMID: 34898376 Free PMC article.
-
A nomogram model based on the number of examined lymph nodes-related signature to predict prognosis and guide clinical therapy in gastric cancer.Front Immunol. 2022 Nov 2;13:947802. doi: 10.3389/fimmu.2022.947802. eCollection 2022. Front Immunol. 2022. PMID: 36405735 Free PMC article.
-
Molecular network-based identification of competing endogenous RNAs and mRNA signatures that predict survival in prostate cancer.J Transl Med. 2018 Oct 4;16(1):274. doi: 10.1186/s12967-018-1637-x. J Transl Med. 2018. PMID: 30286759 Free PMC article.
Cited by
-
Oncogenic mechanisms of COL10A1 in cancer and clinical challenges (Review).Oncol Rep. 2024 Dec;52(6):162. doi: 10.3892/or.2024.8821. Epub 2024 Oct 11. Oncol Rep. 2024. PMID: 39392043 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
