

Ancillary treatment of patients with lung disease due to non-tuberculous mycobacteria: a narrative review
- PMID: 36245600
- PMCID: PMC9562528
- DOI: 10.21037/jtd-22-410
Ancillary treatment of patients with lung disease due to non-tuberculous mycobacteria: a narrative review
Abstract
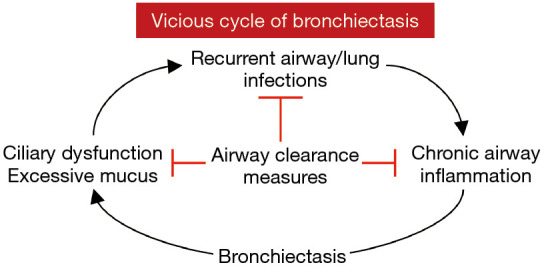
Background and objective: Non-tuberculous mycobacterial lung disease (NTM-LD) manifests with bronchiectasis, inflammatory bronchiolitis, nodules, and/or cavitation. Bronchiectasis is characterized by permanently dilated airways wherein mucus accumulates, creating a vicious cycle of chronic injurious inflammation and recurrent infections. While antibiotics are an important part of the treatment of NTM-LD, airway clearance techniques to mitigate this pathogenic mechanism of bronchiectasis as well as other ancillary measures are also important components of NTM-LD treatment. The objective of this contemporaneous Narrative Review is to emphasize the importance of such ancillary measures.
Methods: We searched PubMed for the key words of "airway clearance", "pulmonary rehabilitation", "nutrition", "swallowing dysfunction", "gastroesophageal reflux", "vestibular dysfunction", or "cochlear dysfunction" with that of "non-tuberculous mycobacterial lung disease", "bronchiectasis", or "respiratory disease". The bibliographies of identified articles were further searched for relevant articles not previously identified. Each relevant article was reviewed by one or more of the authors and a narrative review was composed.
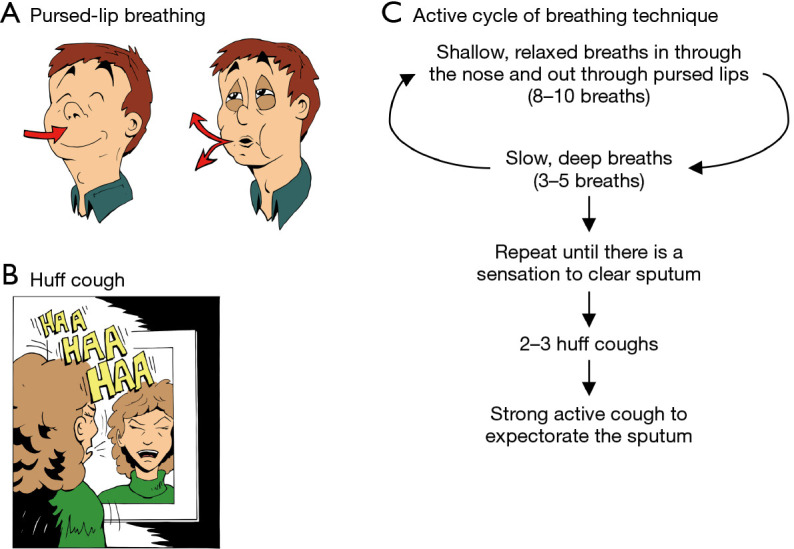
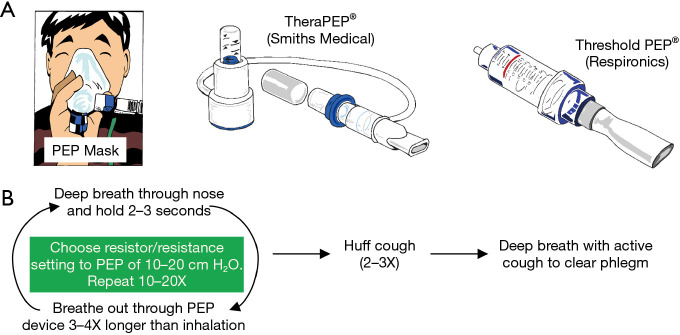
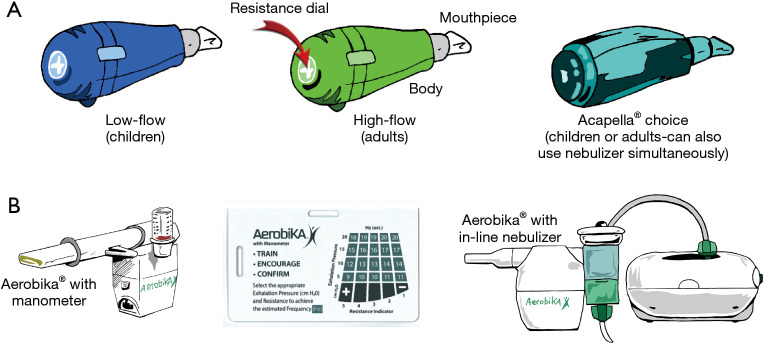
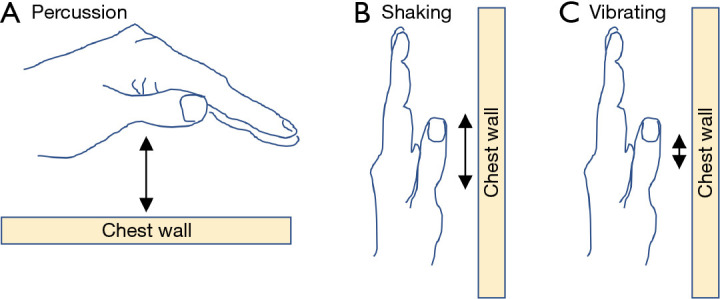
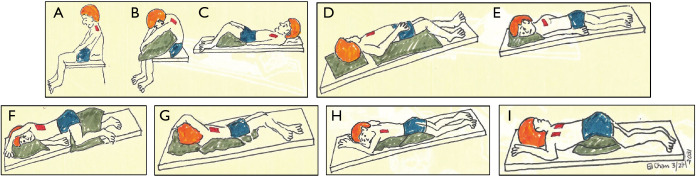
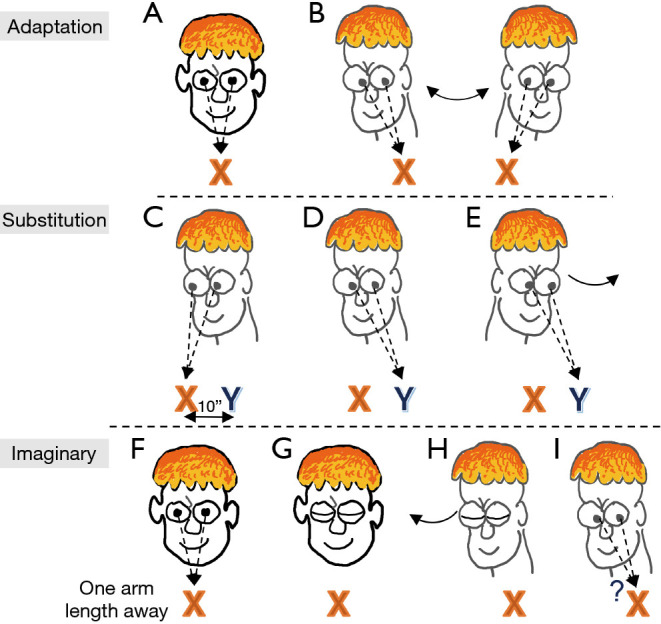
Key content and findings: Herein, we discuss five ancillary treatment measures that are pertinent to patients with bronchiectasis and NTM-LD: (I) airway clearance; (II) physical and pulmonary rehabilitation; (III) nutrition; (IV) diagnosis and mitigation of swallowing dysfunction and of gastroesophageal reflux disease (GERD); and (V) minimization of vestibular and cochlear dysfunction associated with some anti-NTM drugs.
Conclusions: While antibiotics is often the central focus of treatment of NTM-LD, given its propensity for recurrent and recalcitrant infection, other ancillary measures to break the vicious cycle of injurious inflammation and infection should also be emphasized to optimize treatment success.
Keywords: Airway clearance; aspiration; bronchiectasis; gastroesophageal reflux; nutrition; vestibular dysfunction.
2022 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-410/coif). EDC serves as an unpaid editorial board member of Journal of Thoracic Disease from February 2021 to January 2023. The other authors have no conflicts of interest to declare.
Figures

References
-
- Griffith DE. Nontuberculous Mycobacterial Disease: A Comprehensive Approach to Diagnosis and Management. Switzerland: Springer Nature; 2019.
-
- Esposito L. The BE CLEAR Method to Living with Bronchiectasis. New York, NY: Independently Published; 2021.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials