

Intestinal barrier dysfunction is involved in the development of systemic inflammatory responses and lung injury in type A aortic dissection: a case-control study
- PMID: 36245611
- PMCID: PMC9562527
- DOI: 10.21037/jtd-22-1122
Intestinal barrier dysfunction is involved in the development of systemic inflammatory responses and lung injury in type A aortic dissection: a case-control study
Abstract
Background: The definite pathogenesis of lung injury complicated by type A aortic dissection (TAAD) remains unclear. In this paper, we investigated the relationship between intestinal injury, lung injury, and systemic inflammatory responses, with the aim of exploring the mechanism underlying intestinal injury and its impact on systemic inflammatory responses and lung injury in patients with TAAD.
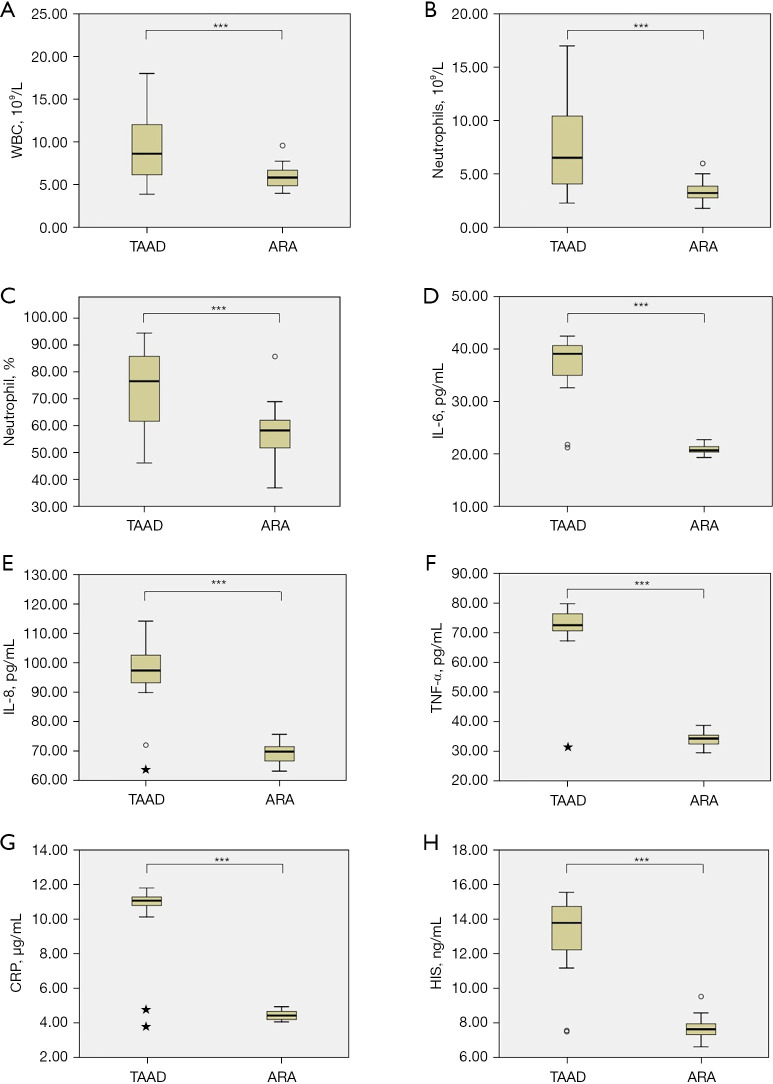
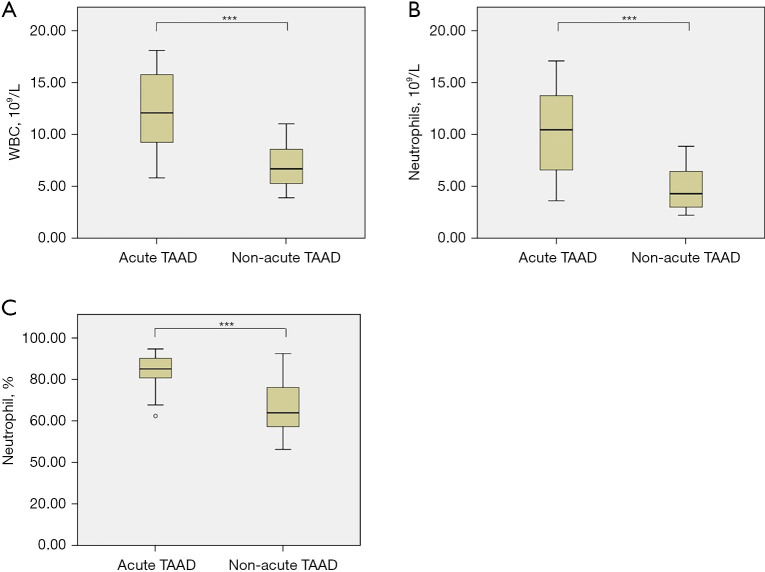
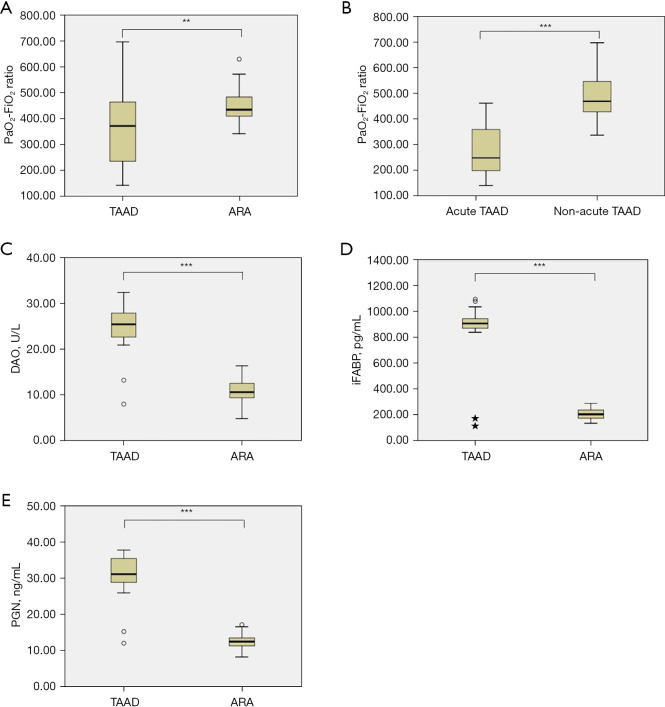
Methods: Patients with TAAD (n=36) and those with aortic root aneurysm (ARA) (n=30) were compared. TAAD patients were younger and had higher creatinine (Cr) than ARA patients. White blood cell (WBC) count, neutrophil count, neutrophil percentage, interleukin (IL)-6, IL-8, tumor necrosis factor α (TNF-α), C-reactive protein (CRP), histamine (HIS) levels, PaO2-FiO2 ratio, diamine oxidase (DAO), intestinal fatty acid binding protein (iFABP), and peptidoglycan (PGN) were measured using the same laboratory methods between the two groups.
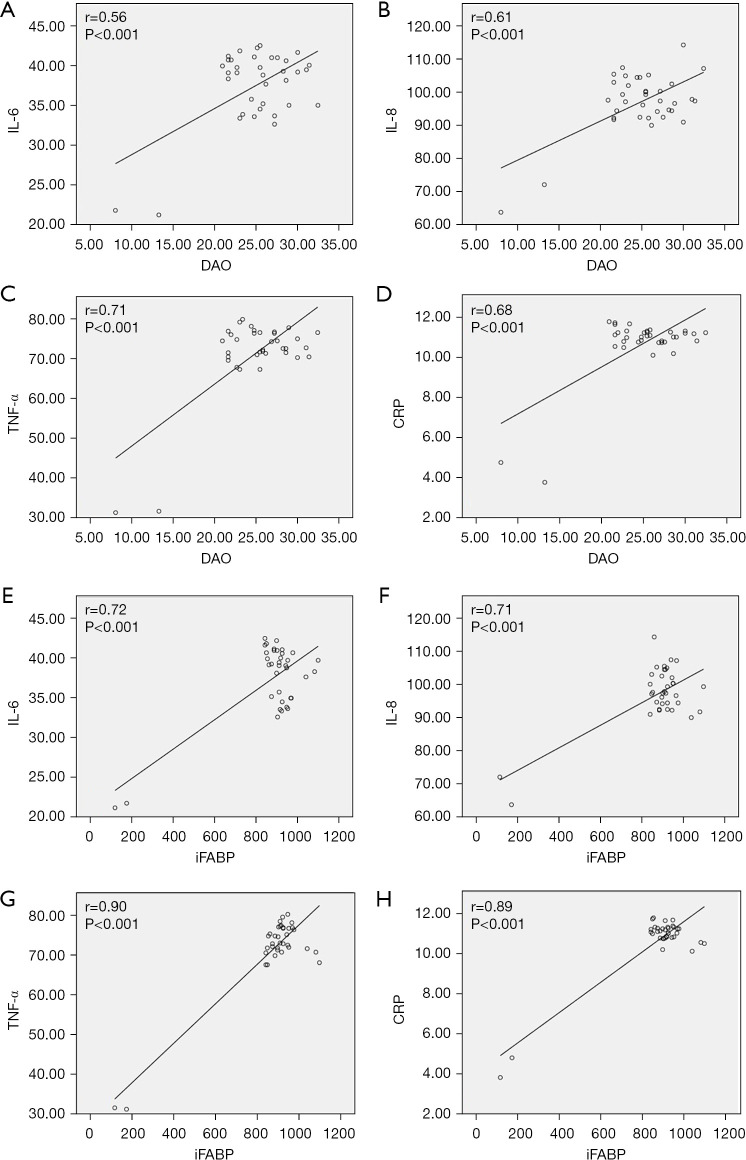
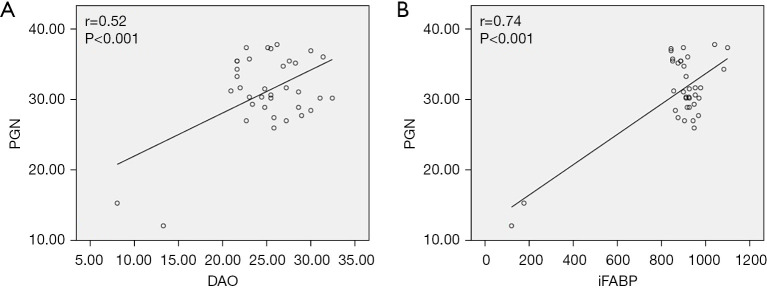
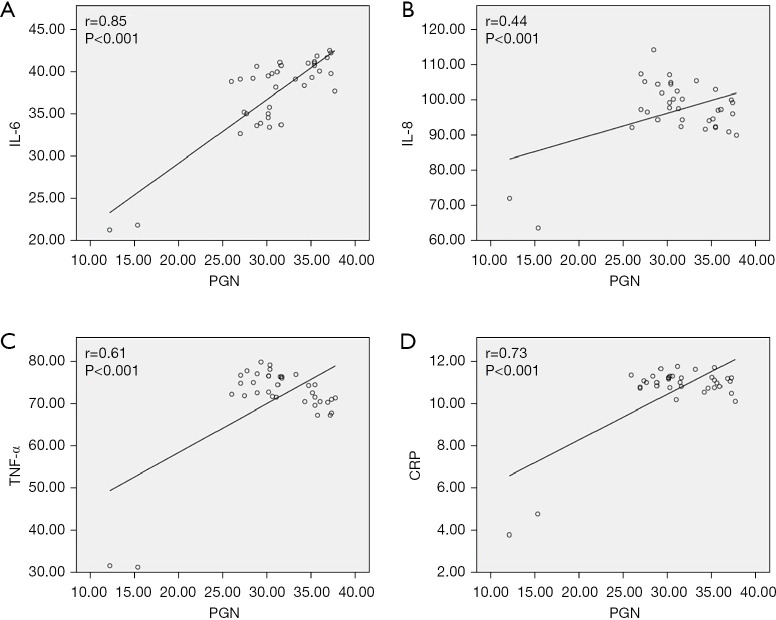
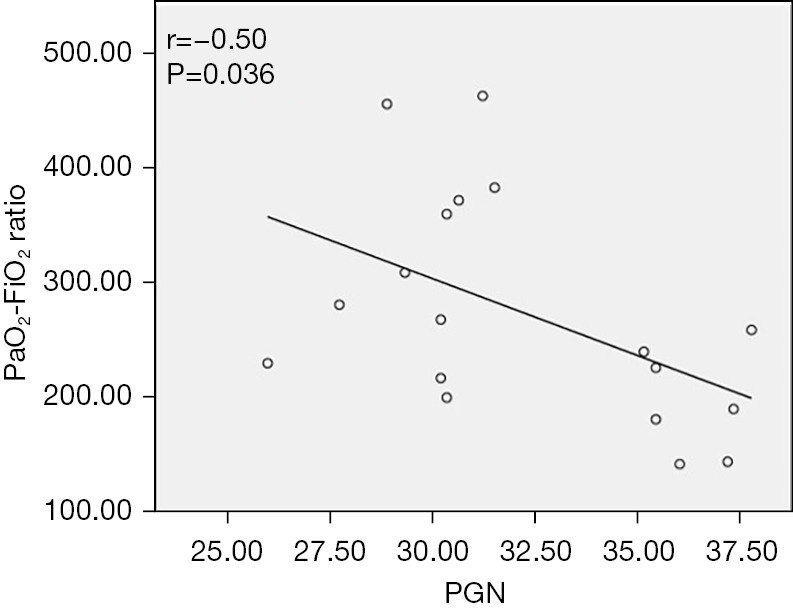
Results: Increased WBC [(9.70±4.05)×109/L vs. (5.88±1.2)×109/L, P<0.001], neutrophil [(7.65±4.27)×109/L vs. (3.40±0.97)×109/L, P<0.001], neutrophil percentage [(74.73±13.42)% vs. (57.67±9.45)%, P<0.001], IL-6 (37.48±4.87 vs. 20.90±0.92 pg/mL, P<0.001), IL-8 (97.15±9.11 vs. 69.46±3.17 pg/mL, P<0.001), TNF-α (71.32±10.35 vs. 33.90±2.27 pg/mL, P<0.001), CRP (10.67±1.62 vs. 4.43±0.26 µg/mL, P<0.001), HIS (13.29±1.88 vs. 7.63±0.58 ng/mL, P<0.001), DAO (24.94±4.72 vs. 10.92±2.44 U/L, P<0.001), iFABP (879.01±190.12 vs. 206.35±42.20 pg/mL, P<0.001), and PGN (31.10±5.51 vs. 12.52±2.20 ng/mL, P<0.001) and decreased PaO2-FiO2 ratio (365.35±146.47 vs. 447.86±70.80 mmHg, P=0.01) were detected in TAAD group relative to ARA group. In TAAD group, positive correlations were detected between DAO and inflammatory cytokines [IL-6 (r=0.56, P<0.001), IL-8 (r=0.61, P<0.001), TNF-α (r=0.71, P<0.001), and CRP (r=0.68, P<0.001)], between iFABP and inflammatory cytokines [IL-6 (r=0.72, P<0.001), IL-8 (r=0.71, P<0.001), TNF-α (r=0.90, P<0.001), and CRP (r=0.89, P<0.001)], between DAO and PGN (r=0.52, P<0.001), between iFABP and PGN (r=0.74, P<0.001), between PGN and inflammatory cytokines [IL-6 (r=0.85, P<0.001), IL-8 (r=0.44, P<0.001), TNF-α (r=0.61, P<0.001), and CRP (r=0.73, P<0.001)]. In acute TAAD subgroup, PGN and PaO2-FiO2 ratio were negatively correlated (r=-0.50, P=0.036).
Conclusions: Systemic inflammatory responses in TAAD patients may lead to lung and intestine injury, and the latter may be involved in the development of systemic inflammatory responses and lung injury in these patients.
Keywords: Type A aortic dissection (TAAD); bacteremia; intestinal injury; lung injury; systemic inflammatory response.
2022 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-1122/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Perioperative dynamic changes of systemic inflammatory response, gut injury, and hypoxemia in patients with acute type-A aortic dissection: an observational case-control study.J Thorac Dis. 2025 Feb 28;17(2):1054-1063. doi: 10.21037/jtd-2025-141. Epub 2025 Feb 27. J Thorac Dis. 2025. PMID: 40083518 Free PMC article.
-
Intestinal Barrier Dysfunction: A Novel Therapeutic Target for Inflammatory Response in Acute Stanford Type A Aortic Dissection.J Cardiovasc Pharmacol Ther. 2016 Jan;21(1):64-9. doi: 10.1177/1074248415581176. Epub 2015 Apr 21. J Cardiovasc Pharmacol Ther. 2016. PMID: 25901009
-
Time-dependent changes of plasma inflammatory biomarkers in type A aortic dissection patients without optimal medical management.J Cardiothorac Surg. 2015 Jan 16;10:3. doi: 10.1186/s13019-014-0199-0. J Cardiothorac Surg. 2015. PMID: 25592634 Free PMC article.
-
Association of plasma diamine oxidase and intestinal fatty acid-binding protein with severity of disease in patient with heat stroke.Am J Emerg Med. 2015 Jul;33(7):867-71. doi: 10.1016/j.ajem.2015.01.047. Epub 2015 Feb 2. Am J Emerg Med. 2015. PMID: 25913083
-
[Relationship between D-dimer concentration and inflammatory factors or organ function in patients with coronavirus disease 2019].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 May;32(5):559-563. doi: 10.3760/cma.j.cn121430-20200414-00518. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 32576347 Chinese.
Cited by
-
Perioperative dynamic changes of systemic inflammatory response, gut injury, and hypoxemia in patients with acute type-A aortic dissection: an observational case-control study.J Thorac Dis. 2025 Feb 28;17(2):1054-1063. doi: 10.21037/jtd-2025-141. Epub 2025 Feb 27. J Thorac Dis. 2025. PMID: 40083518 Free PMC article.
-
Prediction of post-stroke depression with combined blood biomarkers IL-6, TNF-a, and fatty acid binding protein: A prospective study.J Med Biochem. 2023 Oct 27;42(4):638-644. doi: 10.5937/jomb0-43904. J Med Biochem. 2023. PMID: 38084247 Free PMC article.
-
Perioperative oxygenation impairment related to type a aortic dissection.Perfusion. 2025 Jan;40(1):49-60. doi: 10.1177/02676591231224997. Epub 2024 Jan 4. Perfusion. 2025. PMID: 38174389 Free PMC article. Review.
References
-
- Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the diagnosis and management of patients with thoracic aortic disease: Executive summary: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Anesth Analg 2010;111:279-315. 10.1213/ANE.0b013e3181dd869b - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous