

Economic evaluation of microbiological and host biomarker-based tests for the diagnosis of pleural tuberculosis in a high burden setting
- PMID: 36245620
- PMCID: PMC9562520
- DOI: 10.21037/jtd-22-106
Economic evaluation of microbiological and host biomarker-based tests for the diagnosis of pleural tuberculosis in a high burden setting
Abstract
Background: Pleural tuberculosis (TB) remains difficult to diagnose. Tests measuring host biomarkers, such as adenosine deaminase (ADA) and unstimulated interferon-gamma, perform better than conventional microbiological tests for TB diagnosis using pleural fluid. However, there is no data on the cost-effectiveness of these diagnostic approaches.
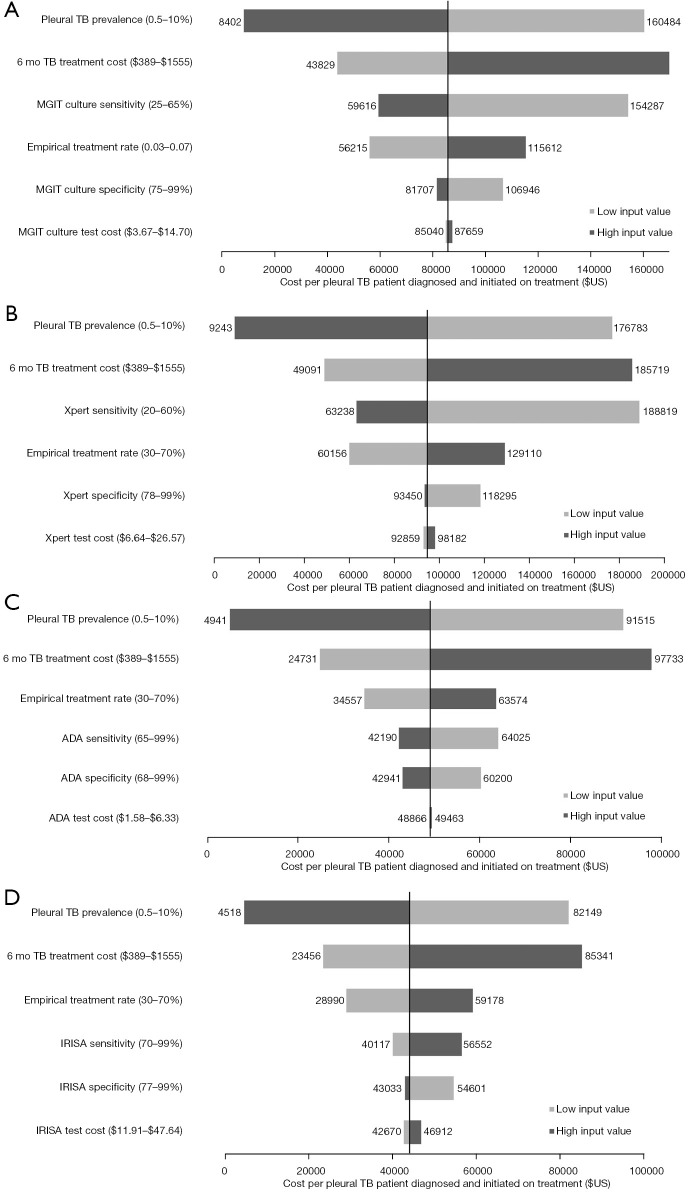
Methods: A cost-consequence analysis was performed from the South African healthcare provider perspective to determine the cost-effectiveness of the following strategies for the diagnosis of pleural TB: (I) Smear microscopy (SM); (II) Mycobacterial-Growth-In-Tube liquid culture (MGIT); (III) adenosine deaminase (ADA); (IV) Xpert ULTRA (Xpert); (V) unstimulated interferon-gamma using IRISA-TB™ (IRISA-TB). Costs (2019 USD) were derived from national sources and outcomes from published literature. Cost-effectiveness was expressed as the cost per pleural TB case diagnosed and initiated on treatment (per 1,000 patients screened). Sensitivity analyses were performed.
Results: Total strategy costs ranged from $354,632 (SM) to $390,363 (ADA). Strategies incorporating highly specific tests, including IRISA-TB and Xpert, had the lowest costs associated with unnecessary treatment. In terms of outcomes (per 1,000 screened), IRISA-TB and ADA correctly identified the most pleural TB cases (8.4 and 8.0 cases, respectively), almost double that of MGIT (4.2 cases) and Xpert ULTRA (3.7 cases). IRISA-TB was the most cost-effective strategy, as the cost per pleural TB patient diagnosed and initiated on treatment was $44,084, ~$5,000 less than ADA (the second most cost-effective strategy; $49,065). These values were most sensitive to changes in pleural TB prevalence, treatment costs, and empirical treatment rates. The cost difference, compared to ADA, equated to a potential saving of ~US$45 million per year in South Africa.
Conclusions: IRISA-TB offers good value for money and is a potentially more cost-effective alternative to ADA for pleural TB diagnosis.
Keywords: Cost-effectiveness; adenosine deaminase; diagnosis; interferon-gamma; pleural tuberculosis.
2022 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-106/coif). Philippa Randall and Rebeng Maine are employees of Antrum Biotech Ltd (developers of the IRISA-TB assay). Anil Pooran received financial support from Antrum Biotech to perform this study. The other authors have no conflicts of interest to declare.
Figures


References
-
- WHO. WHO global tuberculosis report 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/336069/9789240013131-en.... Accessed February 15 2021.
-
- Gounden S, Perumal R, Magula NP. Extrapulmonary tuberculosis in the setting of HIV hyperendemicity at a tertiary hospital in Durban, South Africa. Southern African Journal of Infectious Diseases 2018;33:57-64. 10.1080/23120053.2017.1403207 - DOI
LinkOut - more resources
Full Text Sources
Research Materials