

Urinary Neutrophil Gelatinase-Associated Lipocalin Predicts Intensive Care Unit Admission Diagnosis: A Prospective Cohort Study
- PMID: 36245663
- PMCID: PMC9528386
- DOI: 10.34067/KID.0001492022
Urinary Neutrophil Gelatinase-Associated Lipocalin Predicts Intensive Care Unit Admission Diagnosis: A Prospective Cohort Study
Abstract
Background: Acute kidney injury (AKI) is most commonly caused by tubular injury and is associated with a wide variety of critical illnesses. It is well known that urinary biomarkers can lead to the early identification of AKI. However, the ability of urinary biomarkers to distinguish between different types of critical illness has been less studied.
Methods: In this prospective cohort study, urinary neutrophil gelatinase-associated lipocalin (uNGAL) was measured in 107 patients consecutively admitted to the ICUs in our tertiary medical center. uNGAL samples were collected within 3-6 hours of admission to an ICU and measured by ELISA. All data were analyzed using R statistical software, and univariate analysis was used to determine the correlations of uNGAL levels with AKI stage, admission diagnoses, and ICU course.
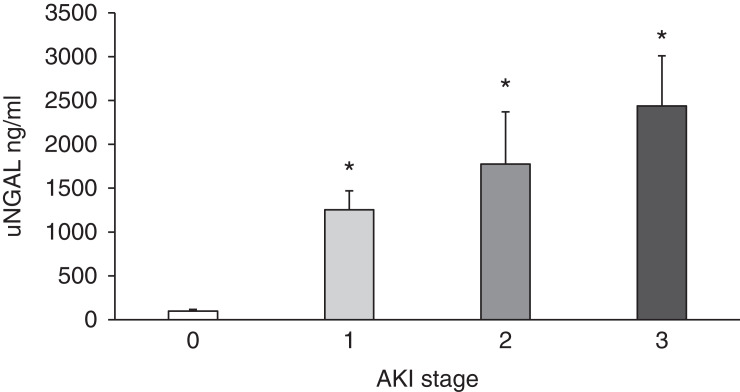
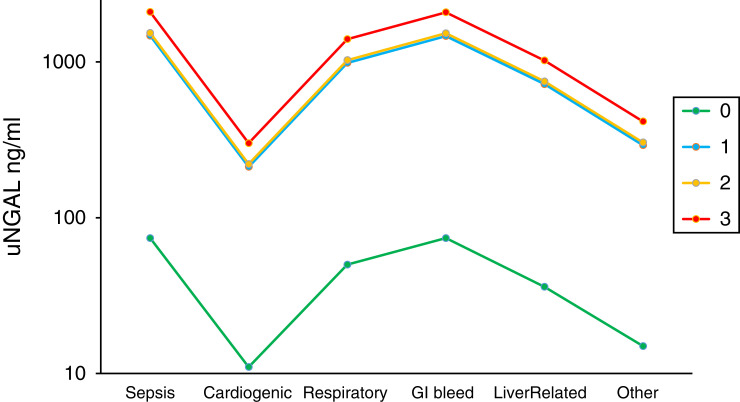
Results: uNGAL level increased by a mean of 24-fold (SD 10-59) in ICU patients with AKI and demonstrated a significant correlation with the different AKI stages. uNGAL predicted the need for RRT, with values increased by more than 15-fold (P<0.05) in patients needing RRT, and remained a useful tool to predict AKI in ICU patients with a urinary tract infection. uNGAL level was correlated with certain ICU admitting diagnoses whereby uNGAL levels were lower in ICU patients with cardiogenic shock compared with other admission diagnoses (β=-1.92, P<0.05).
Conclusions: uNGAL can be used as an early predictor of AKI and its severity in patients admitted to the ICU, including the need for RRT. uNGAL may also help in distinguishing patients with cardiogenic shock from those with other critical illnesses and identifying those at risk for poor outcomes irrespective of the presence of AKI.
Keywords: AKI; ICU nephrology; NGAL; acute kidney injury; acute kidney injury and ICU nephrology; cardiogenic shock; injury marker; lipocalin-2; sepsis; shock; urine biomarker.
Copyright © 2022 by the American Society of Nephrology.
Conflict of interest statement
D.L. Broyles reports being an employer of Dennis Broyles IVD Consulting; consultancy for L3 Healthcare; and ownership interest in Beckman Coulter. M. Malinchoc reports being an employee of L3 Healthcare. D. Oxman reports that his spouse is a full-time employee of Merck working on pediatric vaccines. She works on a number of clinical trials sponsored by Merck. None of these trials have anything to do with the contents of the submitted manuscript. All remaining authors have nothing to disclose.
Figures



References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
