

Improving indicator-condition guided testing for HIV in the hospital setting (PROTEST 2·0): A multicenter, interrupted time-series analysis
- PMID: 36246146
- PMCID: PMC9558045
- DOI: 10.1016/j.lanepe.2022.100515
Improving indicator-condition guided testing for HIV in the hospital setting (PROTEST 2·0): A multicenter, interrupted time-series analysis
Abstract
Background: Indicator-condition (IC) guided HIV testing is a feasible and cost-effective strategy to identify undiagnosed people living with HIV (PLHIV), but remains insufficiently implemented. We aimed to promote IC-guided HIV testing in seven ICs.
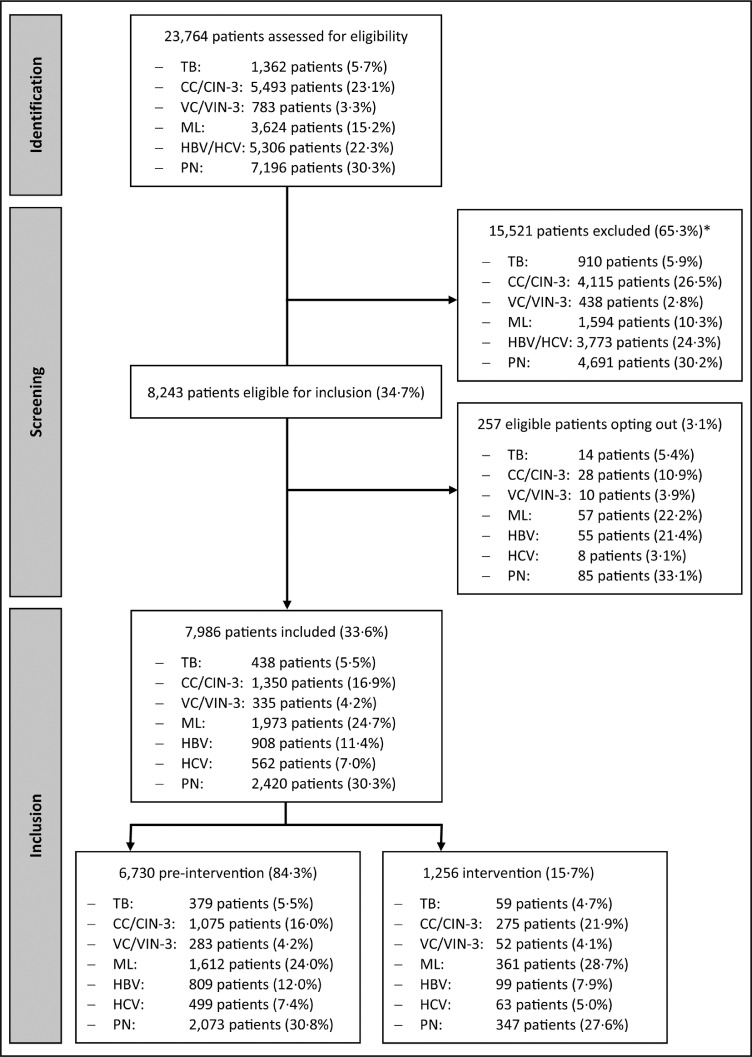
Methods: Relevant departments in five hospitals of the Amsterdam region participated. HIV testing among adult patients without known HIV infection but with an IC was assessed using electronic health records during pre-intervention (January 2015-June 2020) and intervention (July 2020-June 2021) periods. The multifaceted intervention included audit and feedback. The primary endpoint was HIV testing ≤3 months before or after IC diagnosis and the effect of the intervention was evaluated using segmented Poisson regression.
Findings: Data from 7986 patients were included, of whom 6730 (84·3%) were diagnosed with an IC in the pre-intervention period and 1256 (15·7%) in the intervention period. The proportion HIV tested ≤3 months before or after IC diagnosis increased from 36.8% to 47.0% (adjusted risk ratio [RR]= 1.16, 95% CI=1.03-1.30, p=0.02). For individual ICs, we observed significant increases in HIV testing among patients with cervical cancer or intraepithelial neoplasia grade 3 (adjusted RR=3.62, 95% CI=1.93-6.79) and peripheral neuropathy (adjusted RR=2.27 95% CI=1.48-3.49), but not the other ICs. Eighteen of 3068 tested patients were HIV positive (0.6%).
Interpretation: Overall IC-guided testing improved after the intervention, but not for all ICs. Variations in effect by IC may have been due to variations in implemented developments, but the effect of separate elements could not be assessed.
Funding: HIV Transmission Elimination Amsterdam (H-TEAM) initiative, Aidsfonds (grant number: P-42702).
Keywords: Cervical carcinoma; Cervical dysplasia; Diagnostics; HIV; HIV testing; Hepatitis B; Hepatitis C; Indicator condition; Intervention; Lymphoma; Medical education; Neuropathy; Tuberculosis; Vulvar carcinoma; Vulvar dysplasia.
© 2022 The Author(s).
Conflict of interest statement
Dr. Bogers has nothing to disclose. Dr. Schim van der Loeff has nothing to disclose. Dr. Boyd reports grants or contracts: ANRS, ZonMW and Participation on the Data Safety Monitoring Board or Advisory Board: Amsterdam University Medical Centers, Inserm. Dr. Davidovich has nothing to disclose. Dr. van der Valk reports grants or contracts: ViiV Healthcare, Gilead Sciences and Participation on the Data Safety Monitoring Board or Advisory Board: Viiv Healthcare, Gilead Sciences, MSD. Reimbursement paid to institution, and Leadership or fiduciary role in other board, society, committee or advocacy group, paid or unpaid: Member EACS ART and comorbidities guideline committee. Dr. Brinkman has nothing to disclose. Dr. Sigaloff has nothing to disclose. Dr. Branger has nothing to disclose. Dr. Bokhizzou has nothing to disclose. Dr. de Bree has nothing to disclose. Dr. Reiss reports grants or contracts: Gilead Sciences; ViiV Healthcare; Merck: Investigator-initiated study grants to institution and Participation on the Data Safety Monitoring Board or Advisory Board: Gilead Sciences; ViiV Healthcare; Merck: Honoraria for scientific advisory board participation paid to institution. Dr. van Bergen has nothing to disclose. Dr. Geerlings has nothing to disclose.
Figures

References
-
- Temprano Anrs Study Group, Danel C, Moh R, et al. A trial of early antiretrovirals and isoniazid preventive therapy in Africa. N Engl J Med. 2015;373(9):808–822. - PubMed
-
- Bert F, Gualano MR, Biancone P, et al. Cost-effectiveness of HIV screening in high-income countries: a systematic review. Health Policy. 2018;122(5):533–547. - PubMed
LinkOut - more resources
Full Text Sources
