

Early Versus Late DNR Orders and its Predictors in a Saudi Arabian ICU: A Descriptive Study
- PMID: 36247060
- PMCID: PMC9555038
- DOI: 10.4103/sjmms.sjmms_141_22
Early Versus Late DNR Orders and its Predictors in a Saudi Arabian ICU: A Descriptive Study
Abstract
Background: Practices of Do-Not-Resuscitate (DNR) orders show discrepancies worldwide, but there are only few such studies from Saudi Arabia.
Objective: To describe the practice of DNR orders in a Saudi Arabian tertiary care ICU.
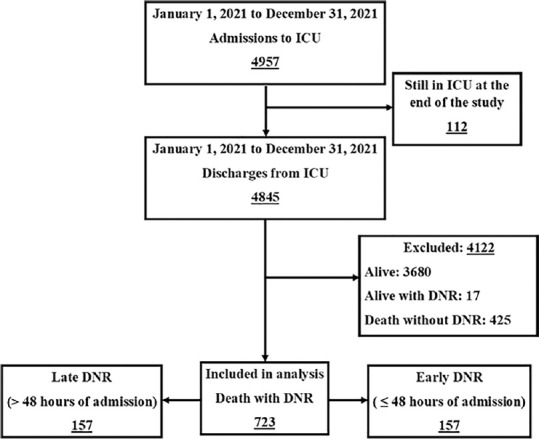
Methods: This retrospective study included all patients who died with a DNR order at the ICU of King Saud Medical City, Riyadh, Saudi Arabia, between January 1 to December 31, 2021. The percentage of early DNR (i.e., ≤48 hours of ICU admission) and late DNR (>48 hours) orders were determined and the variables between the two groups were compared. The determinants of late DNR were also investigated.
Results: A total of 723 cases met the inclusion criteria, representing 14.9% of all ICU discharges and 63% of all ICU deaths during the study period. The late DNR group comprised the majority of the cases (78.3%), and included significantly more patients with acute respiratory distress syndrome (ARDS), community acquired pneumonia (CAP), acute kidney injury, and COVID-19, and significantly fewer cases of readmissions and malignancies. Septic shock lowered the odds of a late DNR (OR = 0.4, 95% CI: 0.2-0.9;P= 0.02), while ARDS (OR = 3.3, 95% CI: 2-5.4;P < 0.001), ischemic stroke (OR = 2.5, 95% CI: 1.1-5.4;P= 0.02), and CAP (OR = 2, 95% CI: 1.3-3.1;P= 0.003) increased the odds of a late DNR.
Conclusion: There was a higher frequency of late DNR orders in our study compared to those reported in several studies worldwide. Cases with potential for a favorable outcome were more likely to have a late DNR order, while those with expected poorer outcomes were more likely to have an early DNR order. The discrepancies highlight the need for clearer guidelines to achieve consistency.
Keywords: Do-not-resuscitate; Saudi Arabia; frequency; intensive care unit; resuscitation orders; timing.
Copyright: © 2022 Saudi Journal of Medicine & Medical Sciences.
Conflict of interest statement
There are no conflicts of interest.
Figures

References
-
- Flannery L, Ramjan LM, Peters K. End-of-life decisions in the Intensive Care Unit (ICU) – Exploring the experiences of ICU nurses and doctors – A critical literature review. Aust Crit Care. 2016;29:97–103. - PubMed
-
- Monteiro NF, Simões I, Gaspar I, Carmo E. Do-not-resuscitate and treatment limitation decisions – Six years of experience from a Portuguese general Intensive Care Unit. Rev Assoc Med Bras (1992) 2019;65:1168–73. - PubMed
-
- American Thoracic Society. Withholding and withdrawing life-sustaining therapy. Ann Intern Med. 1991;115:478–85. - PubMed
-
- Guidelines for the appropriate use of do-not-resuscitate orders. Council on Ethical and Judicial Affairs, American Medical Association. JAMA. 1991;265:1868–71. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous