

Radiation exposure during modern therapeutic endoscopic ultrasound procedures and standard alternatives
- PMID: 36247073
- PMCID: PMC9558486
- DOI: 10.1055/a-1853-0451
Radiation exposure during modern therapeutic endoscopic ultrasound procedures and standard alternatives
Abstract
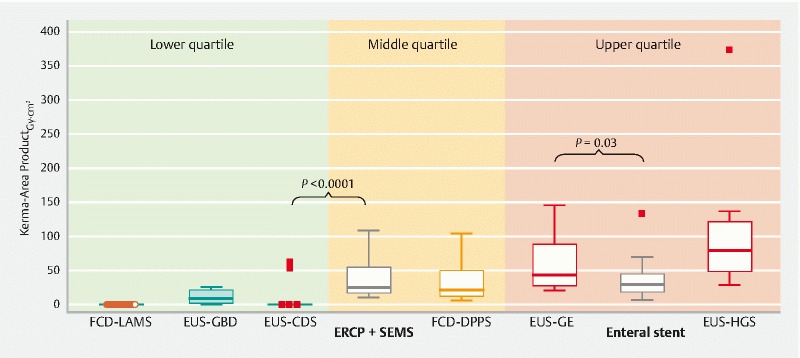
Background and study aims Therapeutic EUS (t-EUS) is increasingly being adopted in clinical practice in tertiary referral centers; however, little is known about radiation exposure (RE) metrics and diagnostic reference limits for it. Methods Kerma-area product (KAP [Gy·cm 2 ]), Air Kerma and fluoroscopy time were retrospectively evaluated for all consecutive t-EUS procedures performed in San Raffaele Institute between 2019 and 2021. For EUS-guided choledochoduodenostomies (EUS-CDS) and gastroenterostomies (EUS-GE), an equal number of endoscopic retrograde cholangiopancreatographies (ERCPs) plus metal stenting and duodenal stents were included respectively for comparison. Results Data from 141 t-EUS procedures were retrieved (49 % pancreatic cancer, 38 % peripancreatic fluid collections). EUS-CDS (N = 44) were mainly performed fluoroless, while ERCPs required a significantly higher RE (KAP = 25 [17-55], P < 0.0001). Fluid collection drainage (EUS-FCD) with lumen apposing metal stents (LAMS, N = 26) were performed fluoroless, while EUS-FCD with double-pigtail plastic stents (DPPS, N = 28) required higher RE (KAP = 23 [13-45]). EUS-guided gallbladder drainage (EUS-GBD, N = 6) required scarce RE (KAP = 9 [3-21]) for coaxial DPPS placement. EUS-GE (N = 27) required higher RE than duodenal stenting (KAP = 44 [28-88] versus 29 [19-46], P = 0.03). EUS-guided hepaticogastrostomies (EUS-HGS, N = 10) had the highest RE among t-EUS procedures (KAP = 81 [49-123]). Procedure complexity or intervening complications were evaluated and resulted in higher RE within each procedure. Conclusions t-EUS procedures have different RE ( P < 0.000001). EUS-CDS, EUS-GBD, and EUS-FCD with LAMS can be performed with no-to-mild radioscopy, unlike standard alternatives. However, radioscopy remains essential in case of technical difficulties or complications. EUS-GE and EUS-HGS involve a high RE. Endoscopists involved in t-EUS might experience RE higher than category standards, which indicates a need for increased awareness and personalized preventive measures.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Competing interests The authors declare that they have no conflict of interest.
Figures

References
-
- Schalk van der Merwe A W, van Wanrooij R LJ, Bronswijk M et al. Therapeutic endoscopic ultrasound: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2022;54:185–205. - PubMed
-
- Vañó E, Miller D L, Martin C J et al. ICRP Publication 135: Diagnostic Reference Levels in Medical Imaging. 2017;46:1–144. - PubMed
LinkOut - more resources
Full Text Sources