

Head-shaking-induced nystagmus reflects dynamic vestibular compensation: A 2-year follow-up study
- PMID: 36247777
- PMCID: PMC9563148
- DOI: 10.3389/fneur.2022.949696
Head-shaking-induced nystagmus reflects dynamic vestibular compensation: A 2-year follow-up study
Abstract
Purpose: We aimed to assess the ability of a head-shaking test (HST) to reflect vestibular compensation in patients after unilateral peripheral vestibular loss and to provide missing evidence and new insights into the features of head-shaking-induced nystagmus (HSN) over a 2-year follow-up.
Background: HSN may occur after a prolonged sinusoidal oscillation of the head. HSN is frequently observed in subjects with vestibular function asymmetry; it usually beats toward the functionally intact or "stronger" ear and can be followed by a reversal of its direction.
Study design: A prospective observational case-control study.
Settings: A tertiary academic referral center.
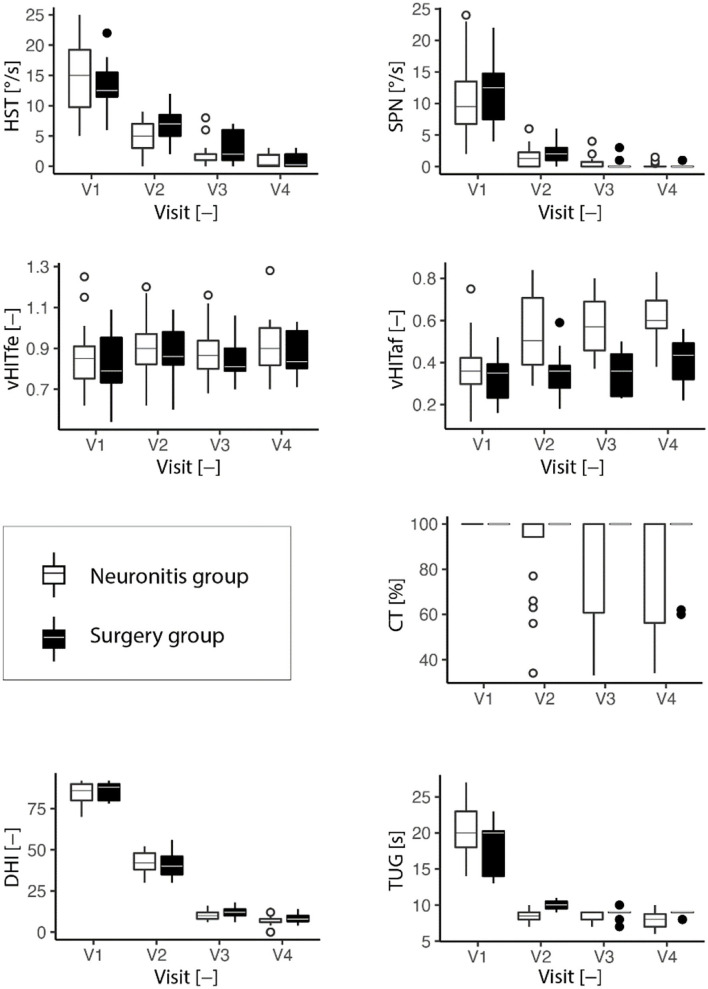
Methods: A total of 38 patients after acute unilateral vestibular loss (22 patients with vestibular neuronitis and 16 patients after vestibular neurectomy) and 28 healthy controls were followed for four consecutive visits over a 2-year period. A complex vestibular assessment was performed on all participants, which included spontaneous nystagmus (SPN), the caloric test, the head-shaking test (HST), the video head impulse test (vHIT), the Timed Up and Go (TUG) test, and the Dizziness Handicap Inventory (DHI) questionnaire. We established the criteria for the poorly compensated group to assess different compensatory behaviors and results.
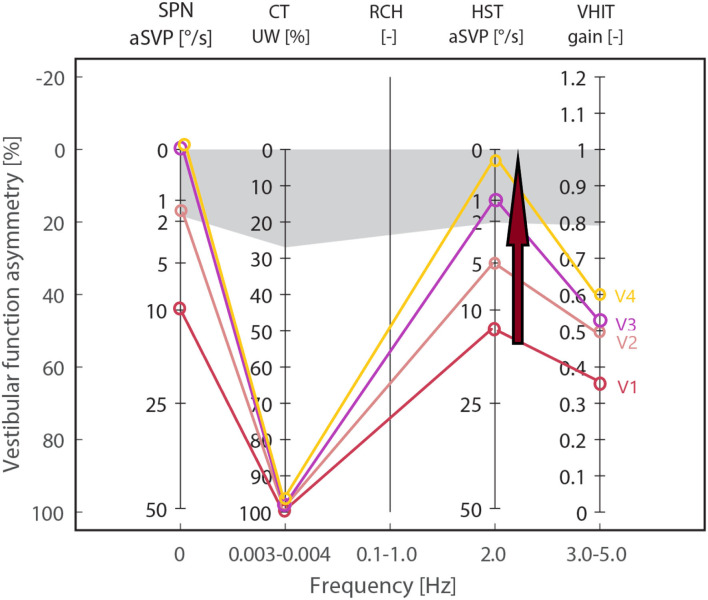
Results: We found a time-related decrease in HSN (ρ < -0.84, p < 0.001) after unilateral vestibular loss. After 2 years of follow-up, HSN intensity in compensated patients reached the level of the control group; TUG and DHI also improved to normal; however, the caloric and vHIT tests remained abnormal throughout all follow-ups, indicating a chronic vestibular deficit. Besides, poorly compensated patients had a well-detectable HSN throughout all follow-ups; TUG remained abnormal, and DHI showed at least a moderate deficit.
Conclusions: Our study showed that, after a unilateral peripheral vestibular loss, the intensity of HSN decreased exponentially over time, reflecting an improvement in dynamic ability and self-perceived deficit. HSN tended to decline to the value of the control group once vestibular compensation was satisfactory and sufficient for a patient's everyday life. In contrast, well-detectable HSN in poorly compensated patients with insufficient clinical recovery confirmed the potential of HSN to reflect and distinguish between adequate and insufficient dynamic compensation. HSN could serve as an objective indicator of stable unilateral vestibular loss.
Keywords: follow-up study; head-shaking nystagmus; head-shaking test; head-shaking-induced nystagmus; velocity storage; vestibular compensation.
Copyright © 2022 Striteska, Valis, Chrobok, Profant, Califano, Syba, Trnkova, Kremlacek and Chovanec.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Head-shaking nystagmus predicts greater disability in unilateral peripheral vestibulopathy.Am J Otolaryngol. 2011 Nov-Dec;32(6):522-7. doi: 10.1016/j.amjoto.2010.11.004. Epub 2011 Feb 8. Am J Otolaryngol. 2011. PMID: 21306790
-
[Further exploration of the classification and clinical value of head-shaking nystagmus].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2023 Jun;37(6):473-477. doi: 10.13201/j.issn.2096-7993.2023.06.013. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2023. PMID: 37253523 Free PMC article. Chinese.
-
Vertical components of head-shaking nystagmus in vestibular neuritis, Meniere's disease and migrainous vertigo.Clin Otolaryngol. 2014 Oct;39(5):261-5. doi: 10.1111/coa.12286. Clin Otolaryngol. 2014. PMID: 25042770
-
Sensitivity and specificity of the head-shaking test for detecting vestibular system abnormalities.Ann Otol Rhinol Laryngol. 1990 Jul;99(7 Pt 1):539-42. doi: 10.1177/000348949009900708. Ann Otol Rhinol Laryngol. 1990. PMID: 2195962 Review.
-
Evolution of Vestibular Findings During and Between the Attacks of Meniere Disease: Update.Neurol Clin Pract. 2024 Apr;14(2):e200235. doi: 10.1212/CPJ.0000000000200235. Epub 2024 Jan 10. Neurol Clin Pract. 2024. PMID: 38223349 Free PMC article. Review.
Cited by
-
The Impact of the Angular Head Movement's Velocity during Diagnostic Maneuvers on Proper Benign Positional Paroxysmal Vertigo Diagnosis and Therapy.Diagnostics (Basel). 2023 Feb 10;13(4):665. doi: 10.3390/diagnostics13040665. Diagnostics (Basel). 2023. PMID: 36832154 Free PMC article.
-
Skull vibration induced nystagmus, velocity storage and self-stability.Front Neurol. 2025 Feb 4;16:1533842. doi: 10.3389/fneur.2025.1533842. eCollection 2025. Front Neurol. 2025. PMID: 39968451 Free PMC article.
-
Evaluation of Semicircular Canal Function Using Video Head Impulse Test in Patients With Peripheral Vestibular Disorders Without Nystagmus.Cureus. 2024 Jun 20;16(6):e62786. doi: 10.7759/cureus.62786. eCollection 2024 Jun. Cureus. 2024. PMID: 39036179 Free PMC article.
References
-
- Bárány R. Untersuchuangen uber das Verhalten des Vestibularapparates bei Kopftraumen und ihre praktische Bedeuntung. (1907). p. 252–66.
-
- Vogel K. Über den nachweis des latenten spontannystagmus. Z Laryng Rhinol. (1932) 22:202–7.
-
- Hain TC. Head-shaking nystagmus and new technology. Neurology. (2007) 68:1333–4. 10.1212/01.wnl.0000261902.31303.cf - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous