

Immunologic aspects of migraine: A review of literature
- PMID: 36247795
- PMCID: PMC9554313
- DOI: 10.3389/fneur.2022.944791
Immunologic aspects of migraine: A review of literature
Abstract
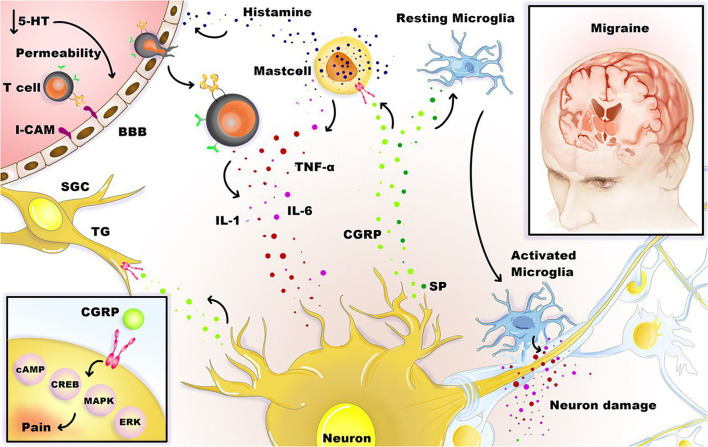
Migraine headaches are highly prevalent, affecting 15% of the population. However, despite many studies to determine this disease's mechanism and efficient management, its pathophysiology has not been fully elucidated. There are suggested hypotheses about the possible mediating role of mast cells, immunoglobulin E, histamine, and cytokines in this disease. A higher incidence of this disease in allergic and asthma patients, reported by several studies, indicates the possible role of brain mast cells located around the brain vessels in this disease. The mast cells are more specifically within the dura and can affect the trigeminal nerve and cervical or sphenopalatine ganglion, triggering the secretion of substances that cause migraine. Neuropeptides such as calcitonin gene-related peptide (CGRP), neurokinin-A, neurotensin (NT), pituitary adenylate-cyclase-activating peptide (PACAP), and substance P (SP) trigger mast cells, and in response, they secrete pro-inflammatory and vasodilatory molecules such as interleukin-6 (IL-6) and vascular endothelial growth factor (VEGF) as a selective result of corticotropin-releasing hormone (CRH) secretion. This stress hormone contributes to migraine or intensifies it. Blocking these pathways using immunologic agents such as CGRP antibody, anti-CGRP receptor antibody, and interleukin-1 beta (IL-1β)/interleukin 1 receptor type 1 (IL-1R1) axis-related agents may be promising as potential prophylactic migraine treatments. This review is going to summarize the immunological aspects of migraine.
Keywords: headache; immunologic aspects; immunological: autoimmune disease; immunology; migraine.
Copyright © 2022 Salahi, Parsa, Nourmohammadi, Razmkhah, Salimi, Rahmani, Zivary, Askarzadeh, Tapak, Vaezi, Sadeghsalehi, Yaghoobpoor, Mottahedi, Garousi and Deravi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
The role of mast cells in migraine pathophysiology.Brain Res Brain Res Rev. 2005 Jul;49(1):65-76. doi: 10.1016/j.brainresrev.2004.11.006. Brain Res Brain Res Rev. 2005. PMID: 15960987 Review.
-
Increase in trigeminal ganglion neurons that respond to both calcitonin gene-related peptide and pituitary adenylate cyclase-activating polypeptide in mouse models of chronic migraine and posttraumatic headache.Pain. 2021 May 1;162(5):1483-1499. doi: 10.1097/j.pain.0000000000002147. Pain. 2021. PMID: 33252452 Free PMC article.
-
Differences in pituitary adenylate cyclase-activating peptide and calcitonin gene-related peptide release in the trigeminovascular system.Cephalalgia. 2020 Oct;40(12):1296-1309. doi: 10.1177/0333102420929026. Epub 2020 Jun 2. Cephalalgia. 2020. PMID: 32486909
-
PACAP-38 but not VIP induces release of CGRP from trigeminal nucleus caudalis via a receptor distinct from the PAC1 receptor.Neuropeptides. 2014 Apr;48(2):53-64. doi: 10.1016/j.npep.2014.01.004. Epub 2014 Jan 25. Neuropeptides. 2014. PMID: 24508136
-
Shared and independent roles of CGRP and PACAP in migraine pathophysiology.J Headache Pain. 2023 Apr 3;24(1):34. doi: 10.1186/s10194-023-01569-2. J Headache Pain. 2023. PMID: 37009867 Free PMC article. Review.
Cited by
-
Increased Prevalence of Headaches and Migraine in Patients with Psoriatic Arthritis and Axial Spondyloarthritis: Insights from an Italian Cohort Study.Biomedicines. 2024 Feb 5;12(2):371. doi: 10.3390/biomedicines12020371. Biomedicines. 2024. PMID: 38397972 Free PMC article.
-
Migraines as a Risk Factor for Many 90-Day Postoperative Complications Following Single-Level Anterior Cervical Diskectomy and Fusion.J Am Acad Orthop Surg Glob Res Rev. 2025 Aug 19;9(8):e25.00060. doi: 10.5435/JAAOSGlobal-D-25-00060. eCollection 2025 Aug 1. J Am Acad Orthop Surg Glob Res Rev. 2025. PMID: 40828986 Free PMC article.
-
Independent causal effect of migraines on Alzheimer's disease risk: a multivariate Mendelian randomization study.Front Neurol. 2024 Jun 5;15:1401880. doi: 10.3389/fneur.2024.1401880. eCollection 2024. Front Neurol. 2024. PMID: 38903170 Free PMC article.
-
Lack of Association between Common LAG3/CD4 Variants and Risk of Migraine.Int J Mol Sci. 2023 Jan 9;24(2):1292. doi: 10.3390/ijms24021292. Int J Mol Sci. 2023. PMID: 36674807 Free PMC article.
-
Decoding migraine disorders: parathyroid hormone-related peptide receptors as key genetic drivers.Brain Commun. 2025 Apr 28;7(2):fcaf142. doi: 10.1093/braincomms/fcaf142. eCollection 2025. Brain Commun. 2025. PMID: 40297711 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials