

Perioperative adverse events in adult and pediatric spine surgery: A prospective cohort analysis of 364 consecutive patients
- PMID: 36248110
- PMCID: PMC9560666
- DOI: 10.1016/j.bas.2021.100858
Perioperative adverse events in adult and pediatric spine surgery: A prospective cohort analysis of 364 consecutive patients
Abstract
Introduction: A precise knowledge of the possible Adverse Events (AEs) related to spinal surgical procedures is crucial in clinical practice.
Research question: Purposes of this study are: to determine the prevalence and severity of perioperative AEs associated with pediatric and adult spine surgery in a high volume center; to estimate the impact of perioperative AEs on length of hospital stay (LOS).
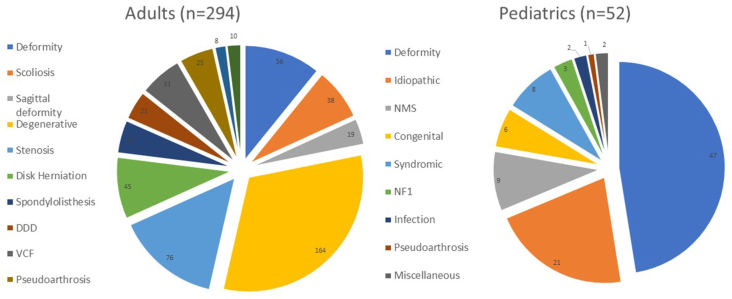
Material and methods: This is a prospective, observational, monocenter study, including 346 consecutive patients (294 adults and 52 pediatrics). The SAVES-V2 questionnaire was used to record AEs. The form was updated by the medical staff every time an adverse event was recorded during hospitalization.
Results: 21,2% of pediatric patients and 20,7% of adults had at least 1 perioperative AEs. In adults, dural tear (3.1%) and neuropathic pain (4,8%), were the most frequent intraoperative and postoperative AE, respectively. In pediatric patients, neurologic deterioration was the most frequent postoperative AE. A diagnosis of deformity (p=0.01), an ASA grade equal or superior to 3 (p=0.023) and the procedure 'Posterior Spinal Fusion' (p=0.001) were associated with a higher frequency of AEs. AEs required prolonged LOS in 40 cases, 7 (70%) pediatric patients and 33 (65%) adults.
Discussion and conclusion: The overall prevalence of AEs is 20.8%, and, although the distribution is almost equal between adult and pediatric patients, their severity is related to age, being higher in pediatric patients. Deformities, deformity correction, revision surgery and AP surgery are the most impactful factors. AEs seriously affect hospitalization, with prolonged LOS (mean 6 days).
Keywords: Adverse events; Deformity; Epidemiology; Patient's Safety; Spine surgery.
© 2021 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Morbidity and mortality of major adult spinal surgery. A prospective cohort analysis of 942 consecutive patients.Spine J. 2012 Jan;12(1):22-34. doi: 10.1016/j.spinee.2011.12.003. Epub 2011 Dec 29. Spine J. 2012. PMID: 22209243
-
An economic evaluation of perioperative adverse events associated with spinal surgery.Spine J. 2013 Jan;13(1):44-53. doi: 10.1016/j.spinee.2013.01.003. Spine J. 2013. PMID: 23384882
-
Generic versus disease-specific adverse event reporting: a comparison of the NSQIP and SAVES databases for the identification of acute care adverse events in adult spine surgery.J Neurosurg Spine. 2023 Apr 28;39(2):263-270. doi: 10.3171/2023.3.SPINE221437. Print 2023 Aug 1. J Neurosurg Spine. 2023. PMID: 37119107
-
Single-dose intravenous ketorolac for acute postoperative pain in adults.Cochrane Database Syst Rev. 2021 May 17;5(5):CD013263. doi: 10.1002/14651858.CD013263.pub2. Cochrane Database Syst Rev. 2021. PMID: 33998669 Free PMC article.
-
Outcome of pediatric patients with severe restrictive lung disease following reconstructive spine surgery.Spine (Phila Pa 1976). 2004 Mar 1;29(5):528-34; discussion 535. doi: 10.1097/01.brs.0000103344.25246.64. Spine (Phila Pa 1976). 2004. PMID: 15129066 Review.
Cited by
-
Prospective insights into spinal surgery outcomes and adverse events: A comparative study between patients 65-79 years vs. ≥80 years from a German tertiary center.Brain Spine. 2024 Feb 17;4:102768. doi: 10.1016/j.bas.2024.102768. eCollection 2024. Brain Spine. 2024. PMID: 38510610 Free PMC article.
-
Factors associated with increased length of stay and risk of complications in 336 patients submitted to spine surgery. The role of a validated capture system (SAVES v2) as a first-line tool to properly face the problem.Eur Spine J. 2024 Mar;33(3):1028-1043. doi: 10.1007/s00586-023-08036-1. Epub 2024 Feb 14. Eur Spine J. 2024. PMID: 38353736
-
Postoperative complications after surgery for lumbar spinal stenosis, assessment using two different data sources.Acta Neurochir (Wien). 2024 Apr 23;166(1):189. doi: 10.1007/s00701-024-06086-y. Acta Neurochir (Wien). 2024. PMID: 38653826 Free PMC article.
-
Adverse events in spine surgery: a prospective analysis at a large tertiary center in Germany.Acta Neurochir (Wien). 2023 Sep;165(9):2689-2697. doi: 10.1007/s00701-023-05752-x. Epub 2023 Aug 9. Acta Neurochir (Wien). 2023. PMID: 37555998 Free PMC article.
References
-
- Bruce J., Russell E.M., Mollison J., Krukowski Z.H. The measurement and monitoring of surgical adverse events. Health Technol. Assess. 2001;5:1–194. - PubMed
-
- Culler S.D., Jevsevar D.S., Shea K.G., et al. Incremental hospital cost and length-of-stay associated with treating adverse events among medicare beneficiaries undergoing lumbar spinal fusion during fiscal year 2013. Spine (Phila Pa 1976) 2016;41:1613–1620. doi: 10.1097/BRS.0000000000001641. - DOI - PubMed
-
- Elder N.C., Dovey S.M. Classification of medical errors and preventable adverse events in primary care: a synthesis of the literature. J. Fam. Pract. 2002;51:927–932. - PubMed
LinkOut - more resources
Full Text Sources
