

Neurosurgery outcomes and complications in a monocentric 7-year patient registry
- PMID: 36248111
- PMCID: PMC9560692
- DOI: 10.1016/j.bas.2022.100860
Neurosurgery outcomes and complications in a monocentric 7-year patient registry
Abstract
Introduction: Capturing adverse events reliably is paramount for clinical practice and research alike. In the era of "big data", prospective registries form the basis of clinical research and quality improvement.
Research question: To present results of long-term implementation of a prospective patient registry, and evaluate the validity of the Clavien-Dindo grade (CDG) to classify complications in neurosurgery.
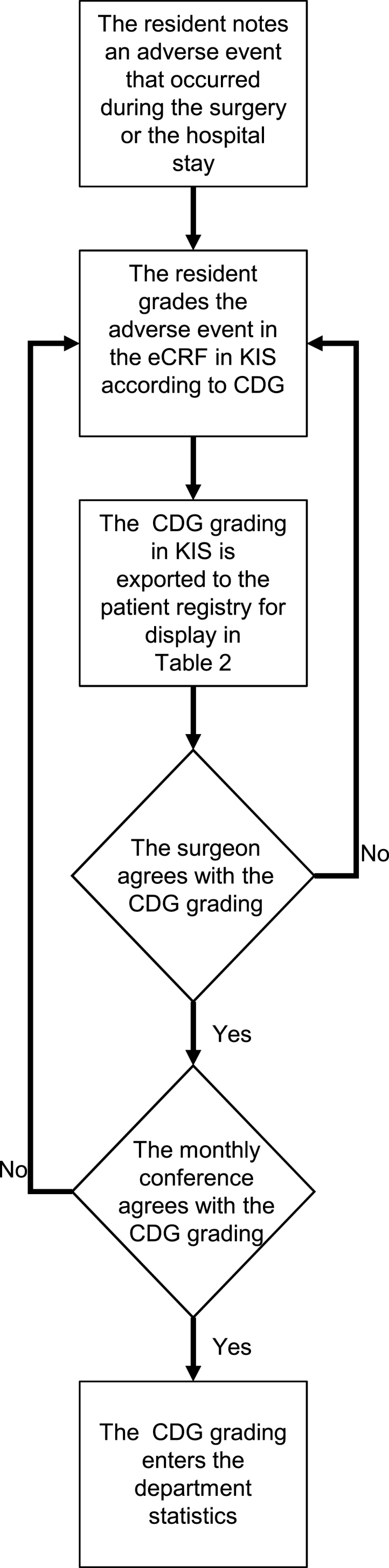
Materials and methods: A prospective registry for cranial and spinal neurosurgical procedures was implemented in 2013. The CDG - a complication grading focused on need for unplanned therapeutic intervention - was used to grade complications. We assess construct validity of the CDG.
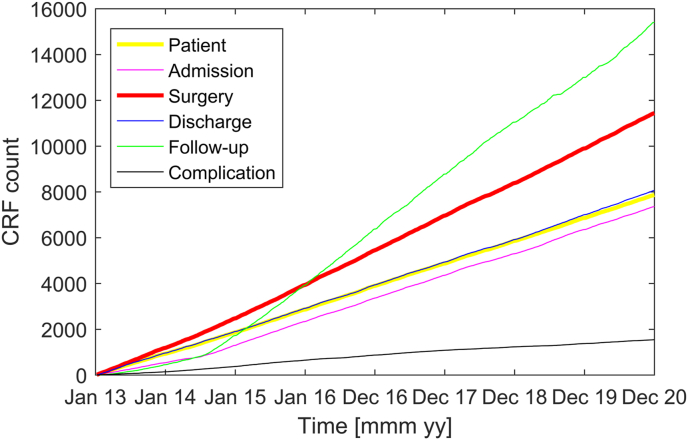
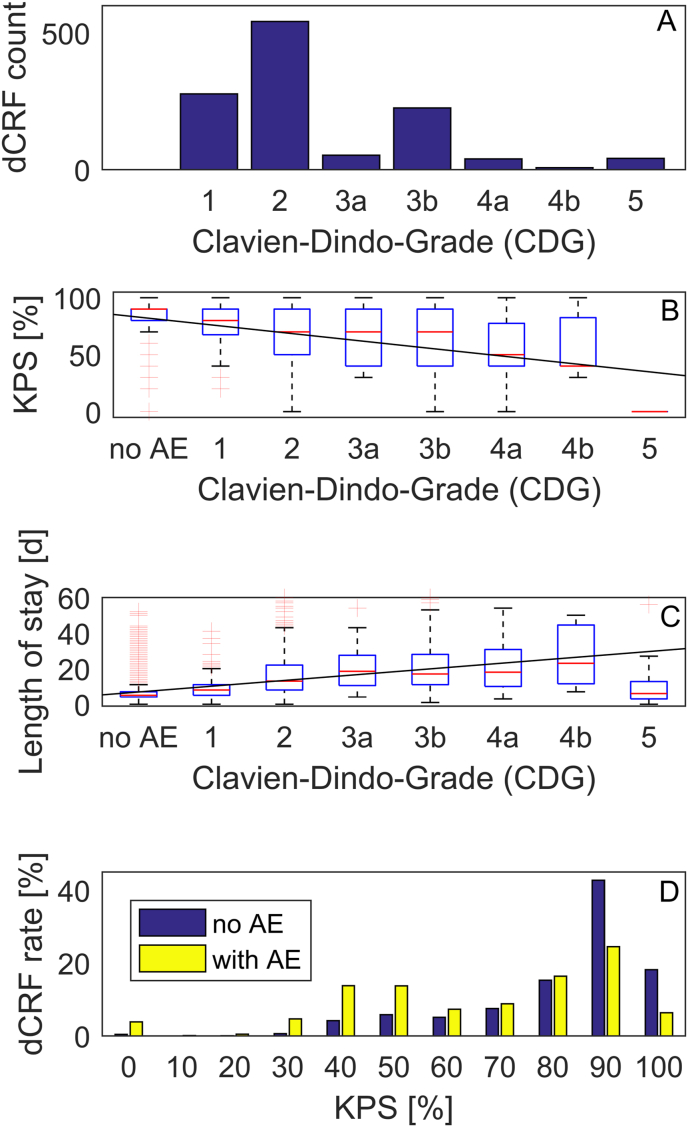
Results: Data acquisition integrated into our hospital workflow permitted to include all eligible patients into the registry. We have registered 8226 patients that were treated in 11994 surgeries and 32494 consultations up until December 2020. Similarly, we have captured 1245 complications on 6308 patient discharge forms (20%) since full operational status of the registry. The majority of complications (819/6308 = 13%) were treated without invasive treatment (CDG 1 or CDG 2). At discharge, there was a clear correlation of CDG and the Karnofsky Performance Status (KPS, rho = -0.29, slope -7 KPS percentage points per increment of CDG) and the length of stay (rho = 0.43, slope 3.2 days per increment of CDG).
Discussion and conclusion: Patient registries with high completeness and objective capturing of complications are central to the process of quality improvement. The CDG demonstrates construct validity as a measure of complication classification in a neurosurgical patient population.
Keywords: Adverse events; Morbidity and mortality rounds; Quality monitoring.
© 2022 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Bai A.D., Dai C., Srivastava S., Smith C.A., Gill S.S. Risk factors, costs and complications of delayed hospital discharge from internal medicine wards at a Canadian academic medical centre: retrospective cohort study. BMC Health Serv. Res. 2019;19(1):935. doi: 10.1186/s12913-019-4760-3. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Medical
