

Assessment of the incidence and nature of adverse events and their association with human error in neurosurgery. A prospective observation
- PMID: 36248119
- PMCID: PMC9560675
- DOI: 10.1016/j.bas.2021.100853
Assessment of the incidence and nature of adverse events and their association with human error in neurosurgery. A prospective observation
Abstract
Introduction: Adverse events in surgery are a relevant cause of costs, disability, or death, and their incidence is a key quality indicator that plays an important role in the future of health care. In neurosurgery, little is known about the frequency of adverse events and the contribution of human error.
Research question: To determine the incidence, nature and severity of adverse events in neurosurgery, and to investigate the contribution of human error.
Material and methods: Prospective observation of all adverse events occurring at an academic neurosurgery referral center focusing on neuro-oncology, cerebrovascular and spinal surgery. All 4176 inpatients treated between September 2019 and September 2020 were included. Adverse events were recorded daily and their nature, severity and a potential contribution of human error were evaluated weekly by all senior neurosurgeons of the department.
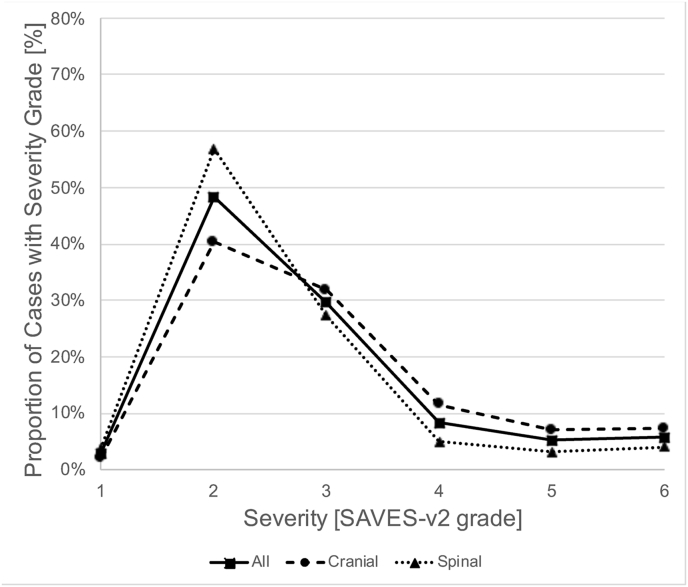
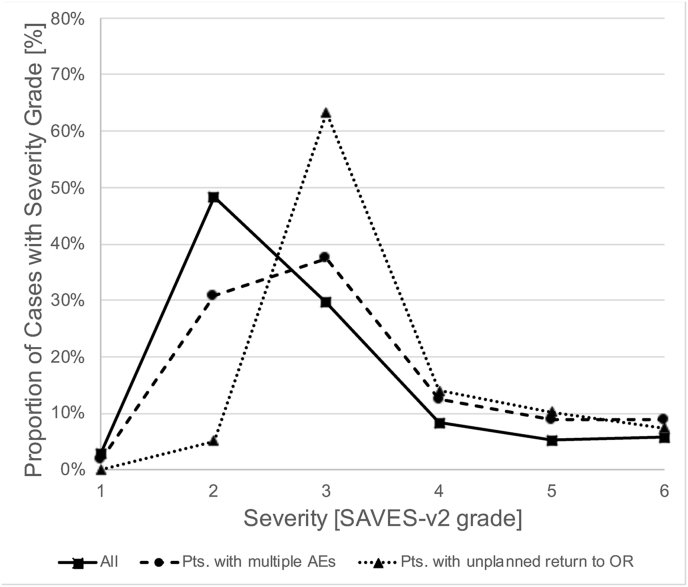
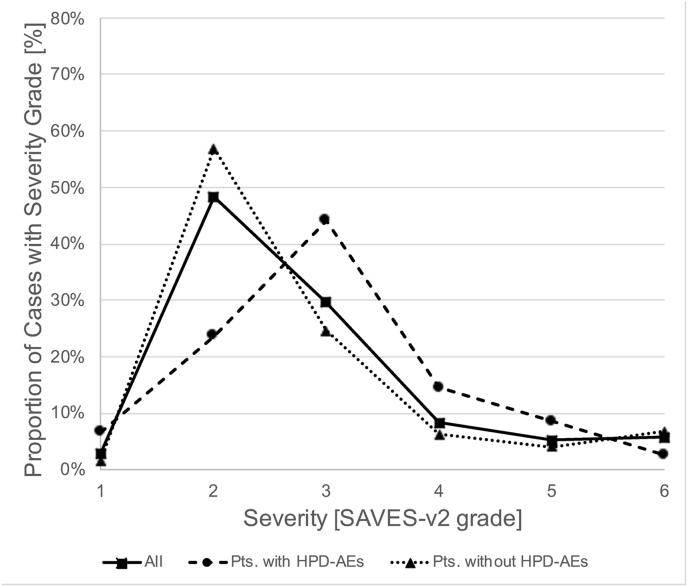
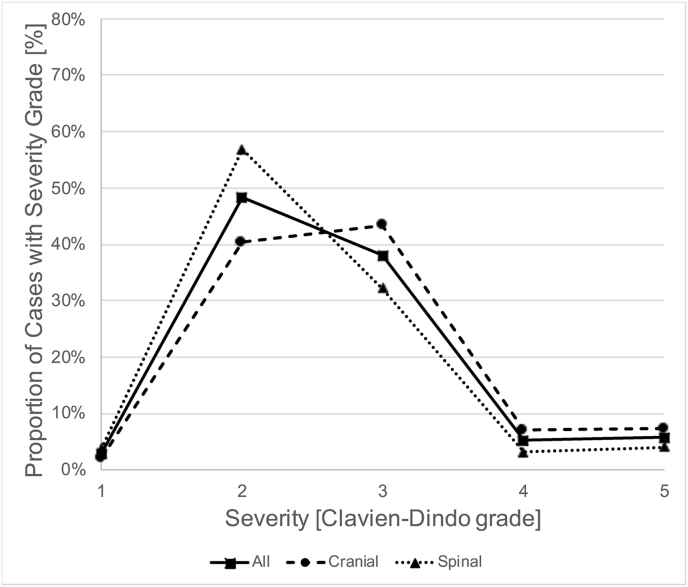
Results: 25.0% of patients had at least one adverse event. In 25.9% of these cases, the major adverse event was associated with human error, mostly with execution (18.3%) or planning (5.6%) deficiencies. 48.8% of cases with adverse events were severe (≥SAVES-v2 grade 3). Patients with multiple adverse events (8.6%) had more severe adverse events (67.6%). Adverse events were more severe in cranial than in spinal neurosurgery (57.6 vs. 39.4%).
Discussion and conclusion: Adverse events occur frequently in neurosurgery. These data can serve as benchmarks when discussing quality-based accreditation and reimbursement in upcoming health care reforms.The high frequency of human performance deficiencies contributing to adverse events shows that there is potential to further eliminate avoidable patient harm.
Keywords: Health care reform; Outcome assessment, Health care; Patient harm; Patient safety; Postoperative complications; Quality indicators, Health Care.
© 2021 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Cohen M.E., Liu Y., Ko C.Y., Hall B.L. Improved surgical outcomes for ACS NSQIP hospitals over time: evaluation of hospital cohorts with up to 8 Years of participation. Ann. Surg. 2016;263(2):267–273. - PubMed
-
- Gawande A.A., Thomas E.J., Zinner M.J., Brennan T.A. The incidence and nature of surgical adverse events in Colorado and Utah in 1992. Surgery. 1999;126(1):66–75. - PubMed
-
- Han S.J., Rolston J.D., Lau C.Y., Berger M.S. Improving patient safety in neurologic surgery. Neurosurg. Clin. 2015;26(2):143–147. vii. - PubMed
LinkOut - more resources
Full Text Sources
