

Clinical adjacent segment pathology after anterior cervical discectomy, with and without fusion, for cervical degenerative disc disease: A single center retrospective cohort study with long-term follow-up
- PMID: 36248168
- PMCID: PMC9560678
- DOI: 10.1016/j.bas.2022.100869
Clinical adjacent segment pathology after anterior cervical discectomy, with and without fusion, for cervical degenerative disc disease: A single center retrospective cohort study with long-term follow-up
Abstract
Introduction: Clinical adjacent segment pathology (CASP) continues to be a cause of concern after anterior surgical treatment for single- or multilevel cervical degenerative disc disease (CDDD). The current literature reports inconsistent incidence rates and contended risk factors in the development of CASP.
Research question: The aim is to determine the incidence of additional CASP-related surgeries after anterior cervical discectomy with fusion (ACDF) or without fusion (ACD) for CDDD. Secondary outcomes include risk factors for the development of CASP and long-term clinical outcomes.
Materials & methods: This is a single-center, retrospective cohort study with a long-term follow up. Patients undergoing ACD(F) for CDDD between January 2012 and December 2019 were included.
Results: A total of 601 patients were included, with an average follow-up period of 5.0 years. Most patients underwent ACDF with stand-alone cages (87.7%). CASP developed in 58 (9.7%) patients, 41 (70.7%) of which required additional adjacent level surgery. ACD significantly accelerated the development of CASP. The C2-C7 Cobb angle appeared less lordotic upon early post-operative imaging in ACDF patients that later-on developed CASP. Baseline degeneration at the index level and adjacent levels was not significantly different between patients with and without CASP.
Discussion & conclusion: In this retrospective cohort, we observe a relatively low rate of additional surgery for CASP in ACDF with stand-alone cages. We suggest that surgical technique, fusion, segmental kyphosis and natural degeneration play a multifactorial role in the development of CASP. Complication rates were low and clinical outcomes were similar for all techniques used.
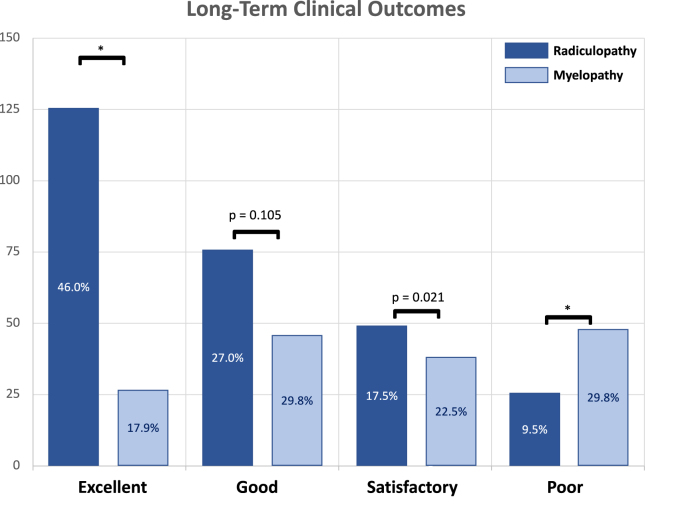
Keywords: Adjacent segment pathology; Anterior cervical discectomy and fusion; Cervical degenerative disc disease; Cervical myelopathy; Cervical radiculopathy.
© 2022 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures




References
-
- Ahn S.-S., Paik H.-K., Chin D.-K., Kim S.-H., Kim D.-W., Ku M.-G. The fate of adjacent segments after anterior cervical discectomy and fusion: the influence of an anterior plate system. World Neurosurg. 2016 May;89:42–50. - PubMed
-
- Bohlman HH, Emery SE, Goodfellow DB, Jones PK. Robinson anterior cervical discectomy and arthrodesis for cervical radiculopathy. Long-term follow-up of one hundred and twenty-two patients. J. Bone Jt. Surg. Am. 75(9):1298–1307. - PubMed
-
- Boogaarts H.D., Bartels R.H.M.A. Prevalence of cervical spondylotic myelopathy. Eur. Spine J. 2015 Apr;2:139–141. 24. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
