

Transformation of neurosurgical training from "see one, do one, teach one" to AR/VR & simulation - A survey by the EANS Young Neurosurgeons
- PMID: 36248173
- PMCID: PMC9560525
- DOI: 10.1016/j.bas.2022.100929
Transformation of neurosurgical training from "see one, do one, teach one" to AR/VR & simulation - A survey by the EANS Young Neurosurgeons
Abstract
Introduction: Modern technologies are increasingly applied in neurosurgical resident training. To date, no data are available regarding how frequently these are used in the training of neurosurgeons, and what the perceived value of this technology is.
Research question: The aim was to benchmark the objective as well as subjective experience with modern- and conventional training technologies.
Material and methods: The EANS Young Neurosurgeons Committee designed a 12-item survey. It was distributed to neurosurgical residents and board-certified neurosurgeons between 6th of February and April 13, 2022.
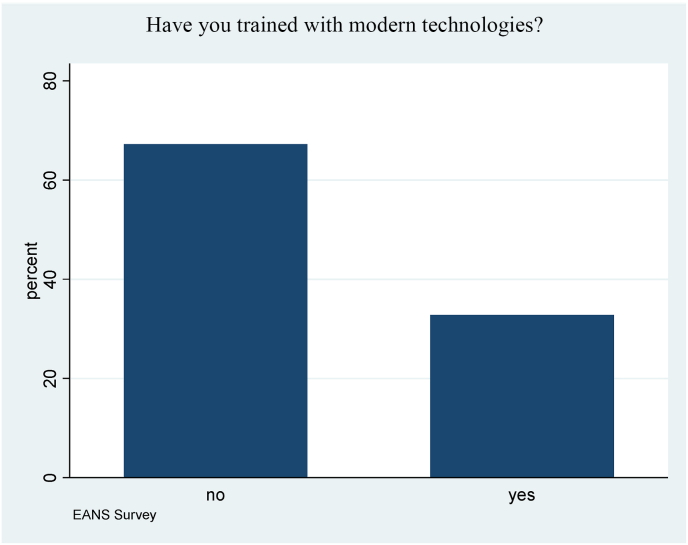
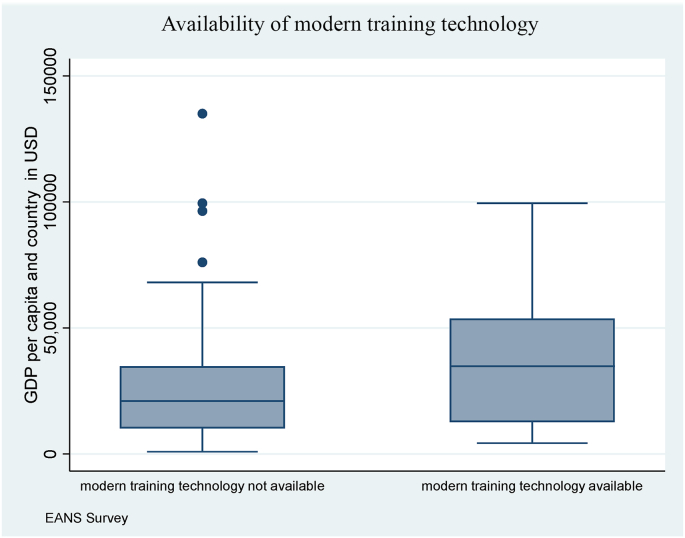
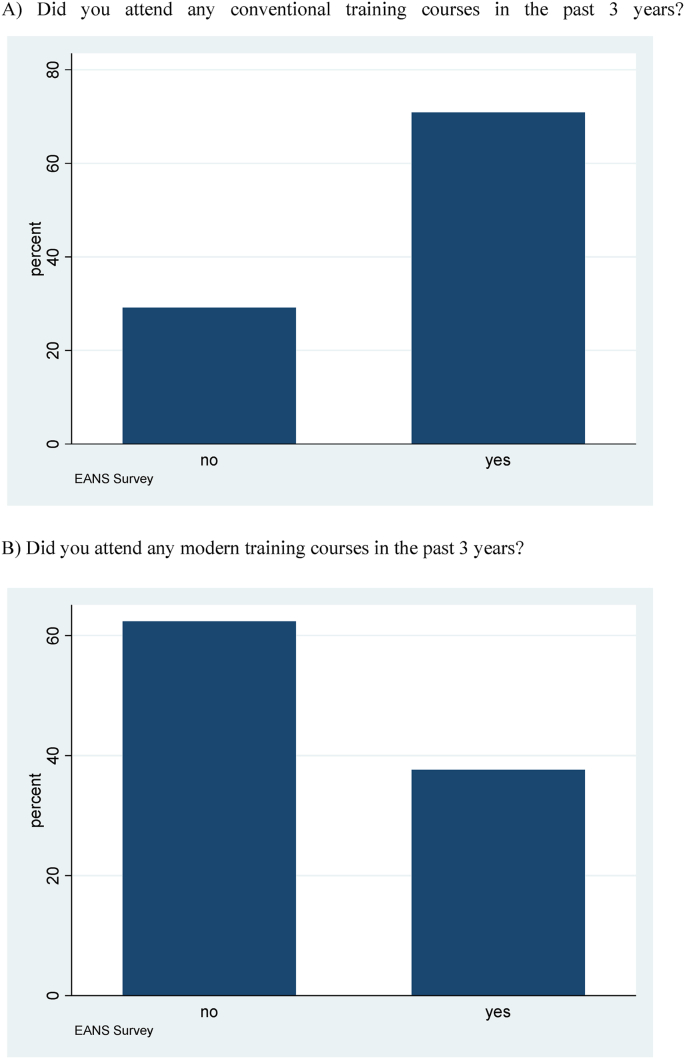
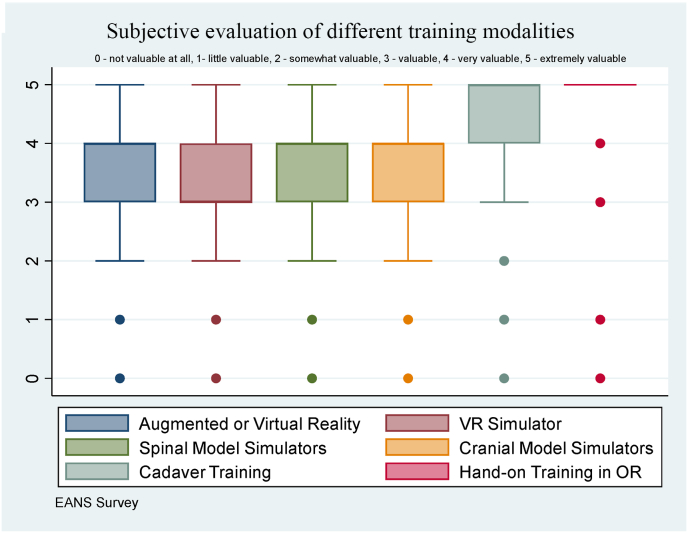
Results: We considered 543 survey responses for analysis. Most participants (67%) indicated not having gained any training experience with modern technology. Most (40.7%) indicated lack of any modern or conventional training technology. Cadaver training was available to 27.6% while all modern training technology to <10%. Participants from countries with high gross domestic product per capita had more access to modern training technologies (p < 0.001). The perceived value of the different technologies was highest for hands-on OR training, followed by cadaver lab. The value of these was rated higher, compared to all modern technologies (p < 0.001).
Discussion and conclusion: Our survey reveals that cadaver labs are used more frequently than modern technologies for today's neurosurgical training. Hands-on training in the operating room (OR) was rated significantly more valuable than any conventional and modern training technology. Our data hence suggest that while modern technologies are well perceived and can surely add to the training of neurosurgeons, it remains critical to ensure sufficient OR exposure.
Keywords: AR/VR; EANS; Neurosurgery; Simulation; Survey; Training.
© 2022 Published by Elsevier B.V. on behalf of EUROSPINE, the Spine Society of Europe, EANS, the European Association of Neurosurgical Societies.
Figures
References
-
- Bernardo A. Virtual reality and simulation in neurosurgical training. World Neurosurg. 2017 Oct;106:1015–1029. - PubMed
-
- Bresler L., Perez M., Hubert J., Henry J.P., Perrenot C. Residency training in robotic surgery: the role of simulation. J. Vis. Surg. 2020 Jun;157(3 Suppl. 2):S123–S129. - PubMed
-
- Chen R., Rodrigues Armijo P., Krause C., SAGES Robotic Task Force. Siu K.-C., Oleynikov D. A comprehensive review of robotic surgery curriculum and training for residents, fellows, and postgraduate surgical education. Surg. Endosc. 2020 Jan;34(1):361–367. - PubMed
-
- Ebner F.H., Dimostheni A., Tatagiba M.S., Roser F. Step-by-step education of the retrosigmoid approach leads to low approach-related morbidity through young residents. Acta Neurochir. 2010 Jun;152(6):985–988. discussion 988. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
