

Association Between Tracheostomy and Functional, Neuropsychological, and Healthcare Utilization Outcomes in the RECOVER Cohort
- PMID: 36248317
- PMCID: PMC9553381
- DOI: 10.1097/CCE.0000000000000768
Association Between Tracheostomy and Functional, Neuropsychological, and Healthcare Utilization Outcomes in the RECOVER Cohort
Abstract
Tracheostomy is commonly performed in critically ill patients requiring prolonged mechanical ventilation (MV). We evaluated the outcomes of tracheostomy in patients who received greater than or equal to 1 week MV and were followed for 1 year.
Design: In this secondary analysis of a prospective observational study, we compared outcomes in tracheostomy versus nontracheostomy patients. Outcomes post ICU included Functional Independence Measure (FIM) subscales, 6-Minute Walk Test (6MWT), Short Form 36 (SF36), Medical Research Council (MRC) Scale, pulmonary function tests (PFTs), Impact of Event Scale (IES), Beck Depression Inventory-II (BDI-II), and vital status and disposition.
Setting: Nine University affiliated ICUs in Canada.
Patients: Medical/surgical patients requiring MV for 7 or more days who were enrolled in the Towards RECOVER Study.
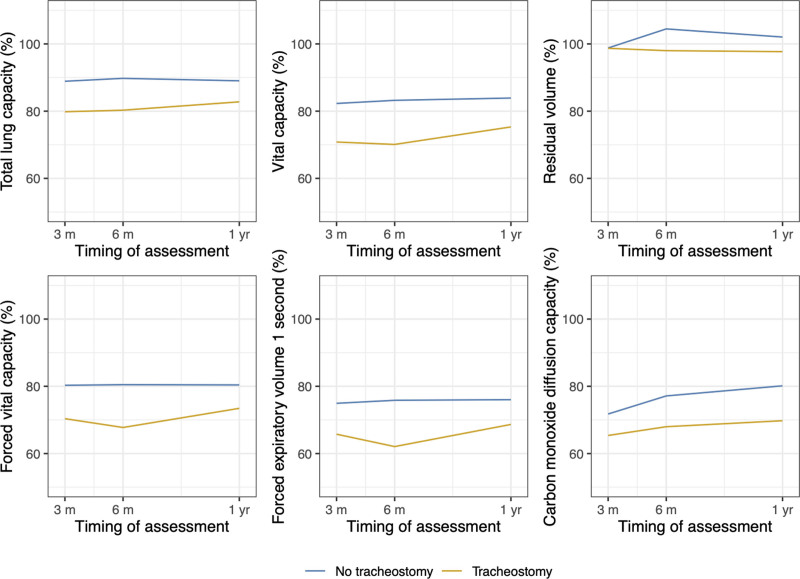
Measurements and main results: Of 398 ICU survivors, 193 (48.5%) received tracheostomy, on median ICU day 14 (interquartile range [IQR], 8-0 d). Patients with tracheostomy were older, had similar severity of illness, had longer MV duration and ICU and hospital stays, and had higher risk of ICU readmission (odds ratio [OR], 1.9; 95% CI, 1.0-3.2) and hospital mortality (OR, 2.6; 95% CI, 1.1-6.1), but not 1-year mortality (hazard ratio, 1.41; 95% CI, 0.88-1.2). Over 1 year, tracheostomy patients had lower FIM-Total (7.7 points; 95% CI, 2.2-13.2); SF36, IES, and BDI-II were similar. From 3 months, tracheostomy patients had 12% lower 6MWT (p = 0.0008) and lower MRC score (3.4 points; p = 0.006). Most PFTs were 5-8% lower in the tracheostomy group. Tracheostomy patients had similar specialist visits (rate ratio, 0.63; 95% CI, 0.28-2.4) and hospital readmissions (OR, 0.82; 95% CI, 0.54-1.3) but were less likely to be at home at hospital discharge and 1 year.
Conclusions: Patients who received tracheostomy had more ICU and hospital care and higher hospital mortality compared with patients who did not receive a tracheostomy. In 1 year follow-up, tracheostomy patients required a higher daily burden of care, expressed by FIM.
Keywords: critical illness; disposition; mechanical ventilation; outcomes; tracheostomy.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
The authors have disclosed that they do not have any potential conflicts of interest.
Figures



References
-
- Siempos II, Ntaidou TK, Filippidis FT, et al. : Effect of early versus late or no tracheostomy on mortality and pneumonia of critically ill patients receiving mechanical ventilation: A systematic review and meta-analysis. Lancet Respir Med 2015; 3:150–158 - PubMed
-
- Scales DC: What’s new with tracheostomy? Intensive Care Med 2013; 39:1005–1008 - PubMed
-
- Trouillet JL, Luyt CE, Guiguet M, et al. : Early percutaneous tracheotomy versus prolonged intubation of mechanically ventilated patients after cardiac surgery: A randomized trial. Ann Intern Med 2011; 154:373–383 - PubMed
-
- Young D, Harrison DA, Cuthbertson BH, et al. ; TracMan Collaborators: Effect of early vs late tracheostomy placement on survival in patients receiving mechanical ventilation: The TracMan randomized trial. JAMA 2013; 309:2121–2129 - PubMed
-
- Herridge MS, Chu LM, Matte A, et al. ; RECOVER Program Investigators (Phase 1: TOWARDs RECOVER); Canadian Critical Care Trials Group: The RECOVER program: Disability risk groups and 1-year outcome after 7 or more days of mechanical ventilation. Am J Respir Crit Care Med 2016; 194:831–844 - PubMed
LinkOut - more resources
Full Text Sources
