

Lymphocyte-C-reactive protein ratio can differentiate disease severity of COVID-19 patients and serve as an assistant screening tool for hospital and ICU admission
- PMID: 36248811
- PMCID: PMC9554799
- DOI: 10.3389/fimmu.2022.957407
Lymphocyte-C-reactive protein ratio can differentiate disease severity of COVID-19 patients and serve as an assistant screening tool for hospital and ICU admission
Abstract
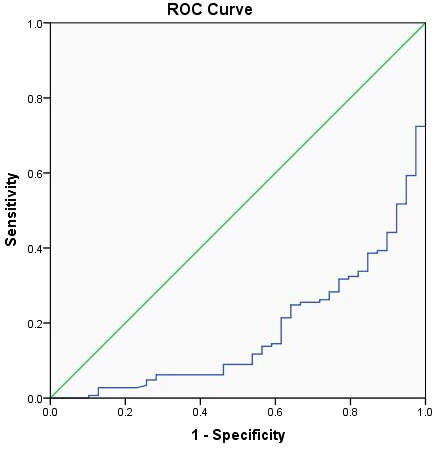
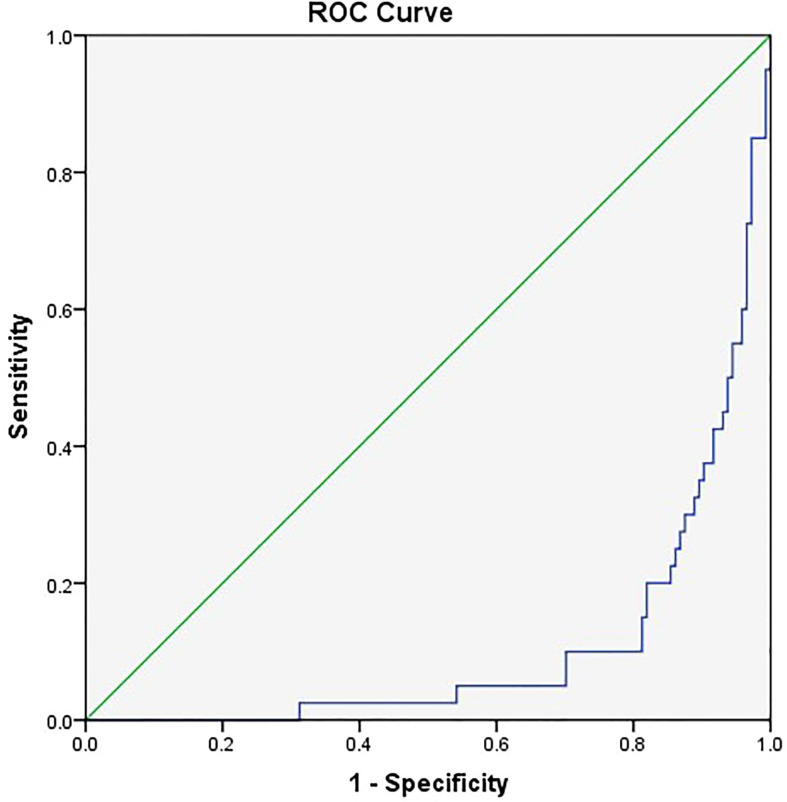
In this study, we aimed to explore whether lymphocyte-C-reactive protein ratio (LCR) can differentiate disease severity of coronavirus disease 2019 (COVID-19) patients and its value as an assistant screening tool for admission to hospital and intensive care unit (ICU). A total of 184 adult COVID-19 patients from the COVID-19 Treatment Center in Heilongjiang Province at the First Affiliated Hospital of Harbin Medical University between January 2020 and March 2021 were included in this study. Patients were divided into asymptomatic infection group, mild group, moderate group, severe group, and critical group according to the Diagnosis and Treatment of New Coronavirus Pneumonia (ninth edition). Demographic and clinical data including gender, age, comorbidities, severity of COVID-19, white blood cell count (WBC), neutrophil proportion (NEUT%), lymphocyte count (LYMPH), lymphocyte percentage (LYM%), red blood cell distribution width (RDW), platelet (PLT), C-reactive protein (CRP), alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum creatinine (SCr), albumin (ALB), total bilirubin (TB), direct bilirubin (DBIL), indirect bilirubin (IBIL), and D-dimer were obtained and collated from medical records at admission, from which sequential organ failure assessment (SOFA) score and LCR were calculated, and all the above indicators were compared among the groups. Multiple clinical parameters, including LYMPH, CRP, and LCR, showed significant differences among the groups. The related factors to classify COVID-19 patients into moderate, severe, and critical groups included age, number of comorbidities, WBC, LCR, and AST. Among these factors, the number of comorbidities showed the greatest effect, and only WBC and LCR were protective factors. The area under the receiver operating characteristic (ROC) curve of LCR to classify COVID-19 patients into moderate, severe, and critical groups was 0.176. The cutoff value of LCR and the sensitivity and specificity of the ROC curve were 1,780.7050 and 84.6% and 66.2%, respectively. The related factors to classify COVID-19 patients into severe and critical groups included the number of comorbidities, PLT, LCR, and SOFA score. Among these factors, SOFA score showed the greatest effect, and LCR was the only protective factor. The area under the ROC curve of LCR to classify COVID-19 patients into severe and critical groups was 0.106. The cutoff value of LCR and the sensitivity and specificity of the ROC curve were 571.2200 and 81.3% and 90.0%, respectively. In summary, LCR can differentiate disease severity of COVID-19 patients and serve as a simple and objective assistant screening tool for hospital and ICU admission.
Keywords: COVID-19; ICU admission; SARS-CoV-2 infection; disease severity; hospital admission; lymphocyte–C-reactive protein ratio; screening tool.
Copyright © 2022 Zhang, Gao, Wang, Li, Du, Tang, Lai, Chen, Yue, Wu, Kang and Zhao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Lymphocyte-C-reactive protein ratio upon admission to predict disease progression and ICU admission in adult patients with diabetic ketoacidosis.Sci Rep. 2025 Jan 23;15(1):3012. doi: 10.1038/s41598-024-84054-3. Sci Rep. 2025. PMID: 39849007 Free PMC article.
-
Dynamic lymphocyte-CRP ratio as a predictor: a single-centre retrospective study on disease severity and progression in adult COVID-19 patients.J Int Med Res. 2024 Mar;52(3):3000605241236278. doi: 10.1177/03000605241236278. J Int Med Res. 2024. PMID: 38483140 Free PMC article.
-
[Relationship between D-dimer concentration and inflammatory factors or organ function in patients with coronavirus disease 2019].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 May;32(5):559-563. doi: 10.3760/cma.j.cn121430-20200414-00518. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 32576347 Chinese.
-
Laboratory features of severe vs. non-severe COVID-19 patients in Asian populations: a systematic review and meta-analysis.Eur J Med Res. 2020 Aug 3;25(1):30. doi: 10.1186/s40001-020-00432-3. Eur J Med Res. 2020. PMID: 32746929 Free PMC article.
-
Meta-analysis investigating the relationship between clinical features, outcomes, and severity of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pneumonia.Am J Infect Control. 2021 Jan;49(1):82-89. doi: 10.1016/j.ajic.2020.06.008. Epub 2020 Jun 12. Am J Infect Control. 2021. PMID: 32540370 Free PMC article. Review.
Cited by
-
Predictive and Prognostic Potentials of Lymphocyte-C-Reactive Protein Ratio Upon Hospitalization in Adult Patients with Acute Pancreatitis.J Inflamm Res. 2024 Mar 13;17:1659-1669. doi: 10.2147/JIR.S450587. eCollection 2024. J Inflamm Res. 2024. PMID: 38504695 Free PMC article.
-
COVID-19 Biomarkers at the Crossroad between Patient Stratification and Targeted Therapy: The Role of Validated and Proposed Parameters.Int J Mol Sci. 2023 Apr 12;24(8):7099. doi: 10.3390/ijms24087099. Int J Mol Sci. 2023. PMID: 37108262 Free PMC article. Review.
-
Presepsin as a prognostic biomarker in COVID-19 patients: combining clinical scoring systems and laboratory inflammatory markers for outcome prediction.Virol J. 2024 Apr 26;21(1):96. doi: 10.1186/s12985-024-02367-1. Virol J. 2024. PMID: 38671532 Free PMC article.
-
Relationship between the lymphocyte to C‑reactive protein ratio and coronary artery disease severity.Exp Ther Med. 2023 Dec 12;27(2):60. doi: 10.3892/etm.2023.12348. eCollection 2024 Feb. Exp Ther Med. 2023. PMID: 38234629 Free PMC article.
-
How Immunonutritional Markers Are Associated with Age, Sex, Body Mass Index and the Most Common Chronic Diseases in the Hospitalized Geriatric Population-A Cross Sectional Study.Nutrients. 2024 Jul 29;16(15):2464. doi: 10.3390/nu16152464. Nutrients. 2024. PMID: 39125344 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous