

Association of perioperative adverse events with subsequent therapy and overall survival in patients with WHO grade III and IV gliomas
- PMID: 36249013
- PMCID: PMC9554557
- DOI: 10.3389/fonc.2022.959072
Association of perioperative adverse events with subsequent therapy and overall survival in patients with WHO grade III and IV gliomas
Abstract
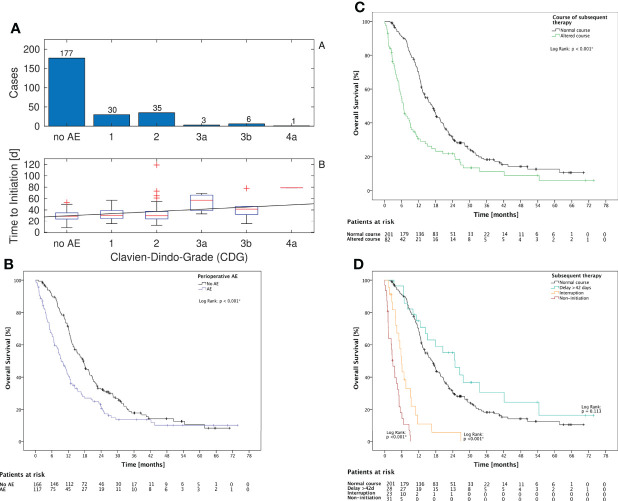
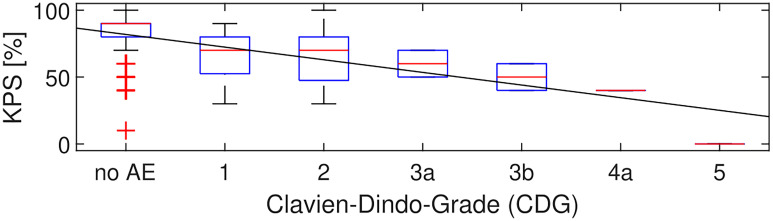
Background: Maximum safe resection followed by chemoradiotherapy as current standard of care for WHO grade III and IV gliomas can be influenced by the occurrence of perioperative adverse events (AE). The aim of this study was to determine the association of AE with the timing and choice of subsequent treatments as well as with overall survival (OS).
Methods: Prospectively collected data of 283 adult patients undergoing surgery for WHO grade III and IV gliomas at the University Hospital Zurich between January 2013 and June 2017 were analyzed. We assessed basic patient characteristics, KPS, extent of resection, and WHO grade, and we classified AE as well as modality, timing of subsequent treatment (delay, interruption, or non-initiation), and OS.
Results: In 117 patients (41%), an AE was documented between surgery and the 3-month follow-up. There was a significant association of AE with an increased time to initiation of subsequent therapy (p = 0.005) and a higher rate of interruption (p < 0.001) or non-initiation (p < 0.001). AE grades correlated with time to initiation of subsequent therapy (p = 0.038). AEs were associated with shorter OS in univariate analysis (p < 0.001).
Conclusion: AEs are associated with delayed and/or altered subsequent therapy and can therefore limit OS. These data emphasize the importance of safety within the maximum-safe-resection concept.
Keywords: adverse events; complications; glioblastoma; high grade glioma; maximum-safe-resection; neurosurgery; subsequent therapy; treatment delay.
Copyright © 2022 Weber, Padevit, Müller, Velz, Vasella, Voglis, Gramatzki, Weller, Regli, Sarnthein and Neidert.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources