

Systemic Factors Associated with a Thinner Choroid in Preterm Infants
- PMID: 36249299
- PMCID: PMC9559969
- DOI: 10.1016/j.xops.2021.100032
Systemic Factors Associated with a Thinner Choroid in Preterm Infants
Abstract
Purpose: To identify systemic health factors associated with a thinner choroid, which has been hypothesized as a cause of poor visual outcomes in low-birth weight infants.
Design: The prospective, observational Study of Eye Imaging in Preterm Infants (BabySTEPS) enrolled infants recommended for retinopathy of prematurity screening based on the American Association of Pediatrics guidelines.
Participants: Infants who underwent imaging with investigational handheld OCT at 36 ± 1 weeks' postmenstrual age (PMA) as part of BabySTEPS.
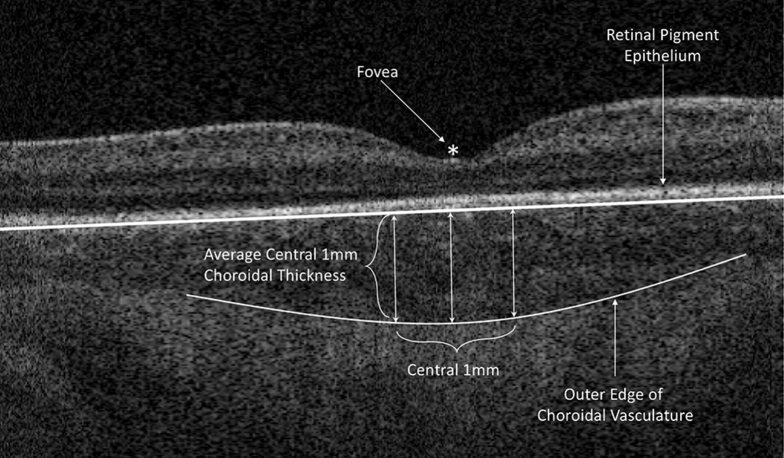
Methods: Average choroidal thickness was measured across the central subfoveal 1 mm. We concurrently collected maternal and infant clinical health data. Univariate and multivariate linear regression analyses were performed to evaluate factors associated with choroidal thickness. The left and right eyes showed similar thicknesses, so their average was used for analysis.
Main outcomes measures: Association between infant health factors and subfoveal choroidal thickness.
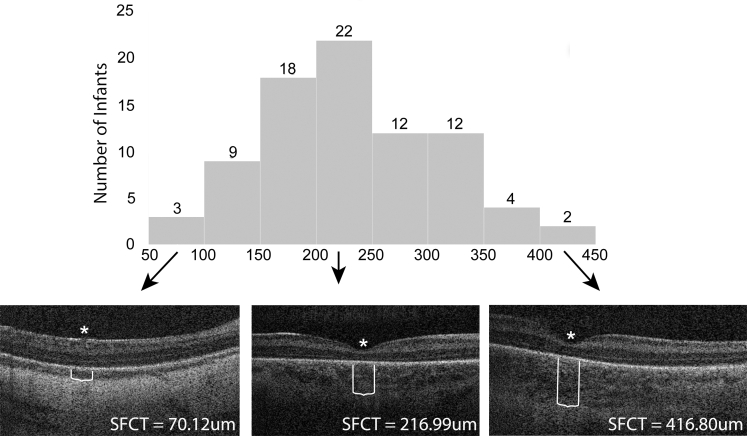
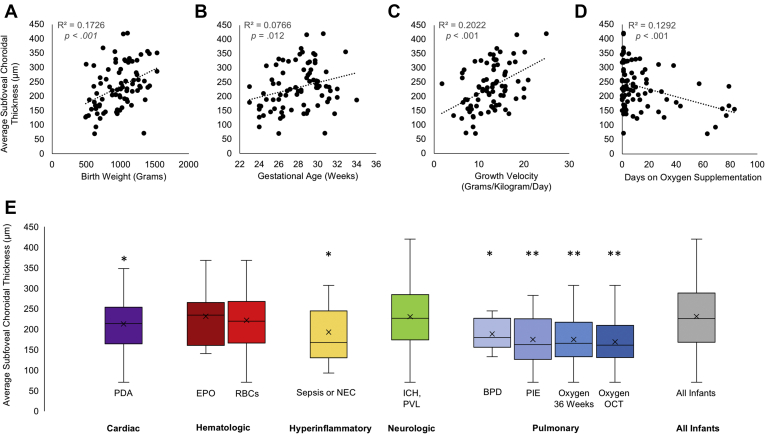
Results: Subfoveal choroidal thickness was measurable in 82 of 85 infants and 94% of eyes. Mean choroidal thickness was 231 ± 78 μm. In the univariate analysis, a thinner choroid was associated with decreased growth velocity (P < 0.001), lower birth weight (P < 0.001), smaller head circumference (P < 0.001), younger gestational age (P = 0.01), the presence of patent ductus arteriosus (P = 0.05), sepsis or necrotizing enterocolitis (P = 0.03), bronchopulmonary dysplasia (P = 0.03), pulmonary interstitial emphysema (P = 0.002), more days on oxygen support (P < 0.001), and being on oxygen support at 36 weeks (P < 0.001) and at the time of imaging (P < 0.001). In the multivariate analysis, growth velocity (P = 0.002) and oxygen support at the time of OCT imaging (P = 0.004) remained associated with a thinner choroid.
Conclusions: A thinner choroid is associated independently with growth velocity and receiving oxygen support at 36 ± 1 weeks PMA. This suggests that choroidal development in preterm infants may be related to growth rate in the first weeks of life and the prolonged use of supplemental oxygen. Longitudinal studies are needed to assess differences in choroidal thickness before 36 weeks PMA and to assess their impact on visual outcomes.
Keywords: BPD, bronchopulmonary dysplasia; BabySTEPS, Study of Eye Imaging in Preterm Infants; Choroid; EPO, erythropoietin administration; ICH, intracranial hemorrhage; ICN, intensive care nursery; Infant; NEC, necrotizing enterocolitis; OCT; Oxygen; PDA, patent ductus arteriosus; PIE, pulmonary interstitial emphysema; PMA, postmenstrual age; PVL, periventricular leukomalacia; RBC, transfusion of packed red blood cells; ROP, retinopathy of prematurity; RPE, retinal pigment epithelium; VEGF, vascular endothelial growth factor; Weight gain.
© 2021 Published by Elsevier Inc. on behalf of the American Academy of Ophthalmology.
Figures
References
-
- Cao J., McLeod S., Merges C.A., Lutty G.A. Choriocapillaris degeneration and related pathologic changes in human diabetic eyes. Arch Ophthalmol. 1998;116(5):589–597. - PubMed
-
- Bourla D.H., Gonzales C.R., Valijan S., et al. Association of systemic risk factors with the progression of laser-treated retinopathy of prematurity to retinal detachment. Retina. 2008;28(3 Suppl):S58–S64. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials
