

Internal Limiting Membrane Peeling and Gas Tamponade For Full-Thickness Macular Holes of Different Etiology - Is It Still Relevant?
- PMID: 36249443
- PMCID: PMC9555881
- DOI: 10.2147/OPTH.S373675
Internal Limiting Membrane Peeling and Gas Tamponade For Full-Thickness Macular Holes of Different Etiology - Is It Still Relevant?
Abstract
Background: Despite the abundance of novel surgical approaches proposed for full thickness macular hole (FTMH) treatment, the choice of the optimal technique remains debatable Vitrectomy with «classic» internal limiting membrane peeling and gas tamponade remains the standard of FTMH surgery in many cases, but there are still very limited recent publications on the outcomes of such surgery.
Purpose: To investigate the anatomical and functional result and to analyze the significance of outcome-related risk factors of the classic 25-gauge pars plana vitrectomy (PPV) with ILM peeling and gas tamponade (GT) for treatment of FTMH of different etiology.
Patients and methods: Thirty-eight eyes of thirty-seven patients with FTMH who underwent 25-gauge PPV, ILM peeling and GT were recruited for this retrospective, consecutive, interventional study. Four eyes with persistent holes underwent a re-operation. Outcome-related factors were discussed.
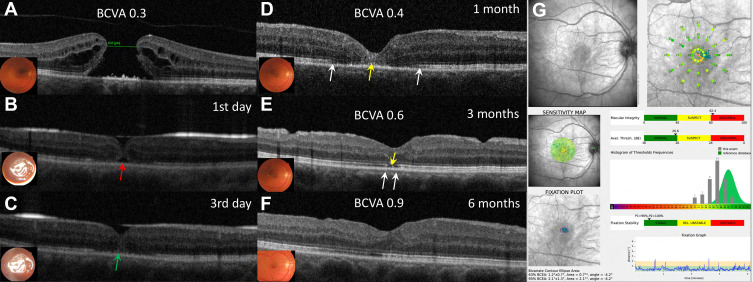
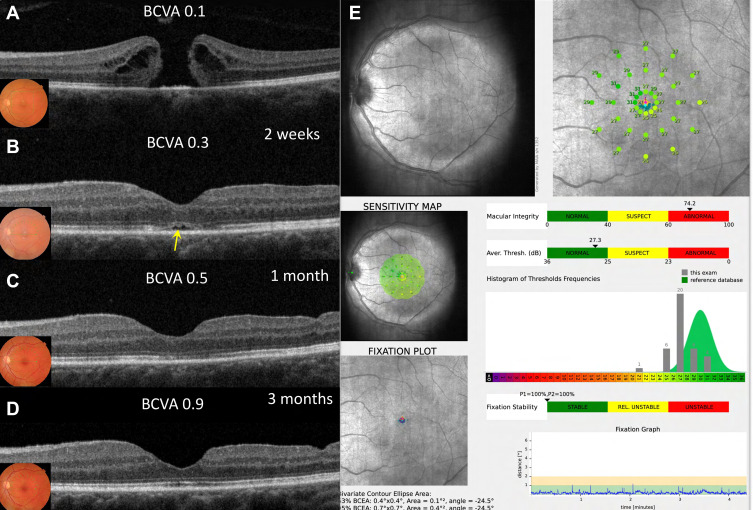
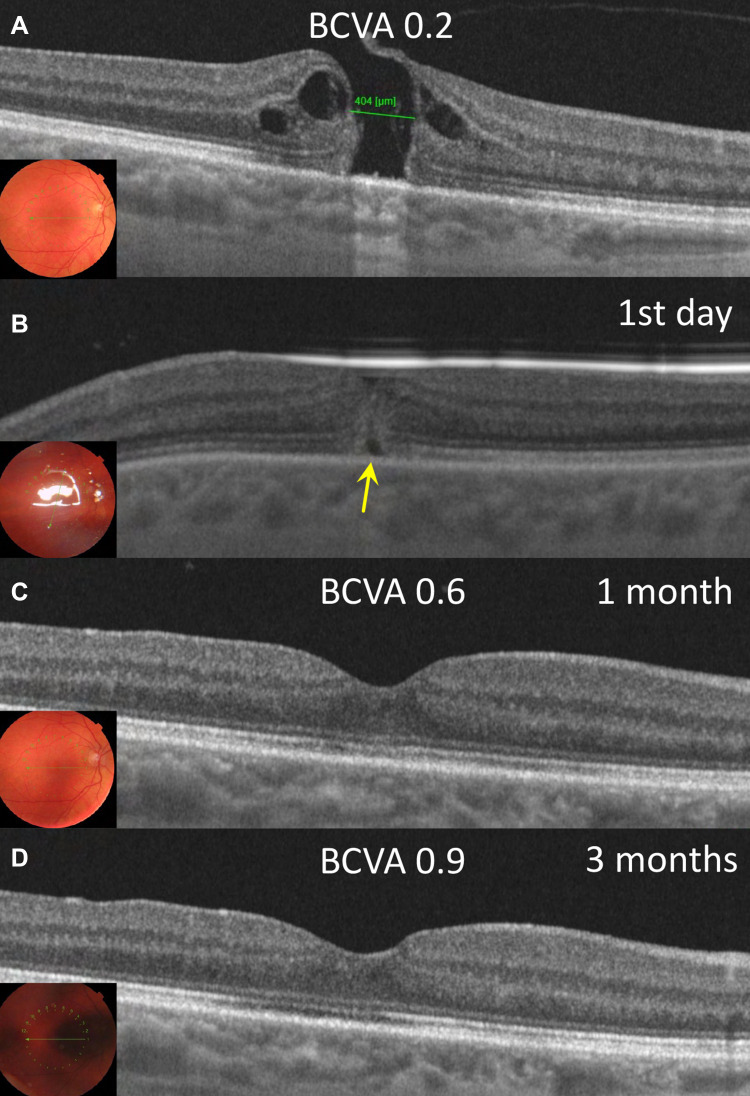
Results: The primary closure rate was 89.5% (34/38). All eyes that underwent the repeated surgery (4 cases) obtained final closure. A hole size of >500 μm has a statistically significant effect on the primary macular hole closure (F = 0.048; φ = 0.38; p ˂ 0.05). In the general group (N = 38), the duration of symptoms directly correlated with age (ρ = 0.34; p = 0.04), size of the hole (ρ = 0.66; p ˂ 0.001) and BCVA before surgery (ρ = 0.59; p ˂ 0.001), after 1 month (ρ = 0.36; p = 0.03), and after 3 months (ρ = 0.35; p = 0.03). Preoperative BCVA was better in initially closed cases (Group 1) (U = 26.0; p = 0.05). In the Group 2 with primary unclosed holes, 75% of the eyes (3/4) had an axial length (AL) >26 mm, while in Group 1 such eyes were 12.5 times less (2/34) 5.9% (F = 0.004; φ = 0.63; р ˂ 0.01). The ELM recovery rate at 3 months was 92% (35/38 eyes) and the restoration of EZ at 3 months was 47% (18/38 eyes). Best-corrected visual acuity of all individuals improved significantly from 0.72 ± 0.35 (logMAR) (Me = 0.7; IQR: 0.5-0.8) to 0.25±0.14 (logMAR) (Me = 0.2; IQR: 0.2 - 0.3) at 1 month and 0.17 ± 0.13 (logMAR) (Me = 0.2; IQR: 0.1 - 0.2) at 3 months after surgery (P = 0.0001).
Conclusion: 25G PPV with ILM and GT for FTMH of different etiology provide satisfactory morphologic and functional outcomes. Elongated AL, large diameter of MH and long duration of symptoms are the risk factors for initial closure. Proper second surgery can obtain satisfactory outcomes for persistent holes.
Keywords: full-thickness macular hole; gas tamponade; internal limiting membrane peeling; macular hole closure; pars plana vitrectomy; restoration of ELM/EZ.
© 2022 Ruban et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest in relation to this work..
Figures
Similar articles
-
Anatomical and functional results after vitrectomy with conventional ILM peeling versus inverted ILM flap technique in large full-thickness macular holes.Int J Retina Vitreous. 2023 Nov 14;9(1):68. doi: 10.1186/s40942-023-00509-1. Int J Retina Vitreous. 2023. PMID: 37964333 Free PMC article.
-
[Functional and Anatomic Outcomes of Primary and Secondary Internal Limiting Membrane Transplantation in Large and Persistent Macular Holes].Klin Monbl Augenheilkd. 2018 Oct;235(10):1159-1164. doi: 10.1055/s-0043-121032. Epub 2017 Nov 20. Klin Monbl Augenheilkd. 2018. PMID: 29156470 German.
-
[Vitrectomy and iOCT-assisted inverted ILM flap technique in patients with full thickness macular holes].Ophthalmologe. 2019 Jul;116(7):617-624. doi: 10.1007/s00347-018-0769-y. Ophthalmologe. 2019. PMID: 30105564 German.
-
Comparative study of vitrectomy combined with internal limiting membrane peeling and vitrectomy combined with internal limiting membrane flap covering in idiopathic macular hole treatment: a meta-analysis and systematic review.Ann Palliat Med. 2021 May;10(5):5474-5482. doi: 10.21037/apm-21-871. Ann Palliat Med. 2021. PMID: 34107705
-
Relaxing Retinotomy in Recurrent and Refractory Full-Thickness Macular Holes: The State of the Art.Life (Basel). 2023 Aug 31;13(9):1844. doi: 10.3390/life13091844. Life (Basel). 2023. PMID: 37763248 Free PMC article. Review.
Cited by
-
Comparison of conventional internal limiting membrane versus pars plana vitrectomy without peeling for small idiopathic macular hole.Int J Retina Vitreous. 2024 Oct 24;10(1):81. doi: 10.1186/s40942-024-00599-5. Int J Retina Vitreous. 2024. PMID: 39449027 Free PMC article.
-
Comments on: Internal Limiting Membrane Peeling and Gas Tamponade for Full-Thickness Macular Holes of Different Etiology - Is It Still Relevant? [Letter].Clin Ophthalmol. 2022 Nov 11;16:3731-3732. doi: 10.2147/OPTH.S396038. eCollection 2022. Clin Ophthalmol. 2022. PMID: 36389635 Free PMC article. No abstract available.
-
Comments on: Internal Limiting Membrane Peeling and Gas Tamponade for Full-Thickness Macular Holes of Different Etiology - Is It Still Relevant? [Response to Letter].Clin Ophthalmol. 2023 Jan 6;17:103-105. doi: 10.2147/OPTH.S402222. eCollection 2023. Clin Ophthalmol. 2023. PMID: 36636618 Free PMC article. No abstract available.
References
-
- Johnson MW, Van Newkirk MR, Meyer KA. Perifoveal vitreous detachment is the primary pathogenic event in idiopathic macular hole formation. Arch Ophthalmol. 2001;119(2):215–222. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
