

A mobile-optimized artificial intelligence system for gestational age and fetal malpresentation assessment
- PMID: 36249461
- PMCID: PMC9553916
- DOI: 10.1038/s43856-022-00194-5
A mobile-optimized artificial intelligence system for gestational age and fetal malpresentation assessment
Abstract
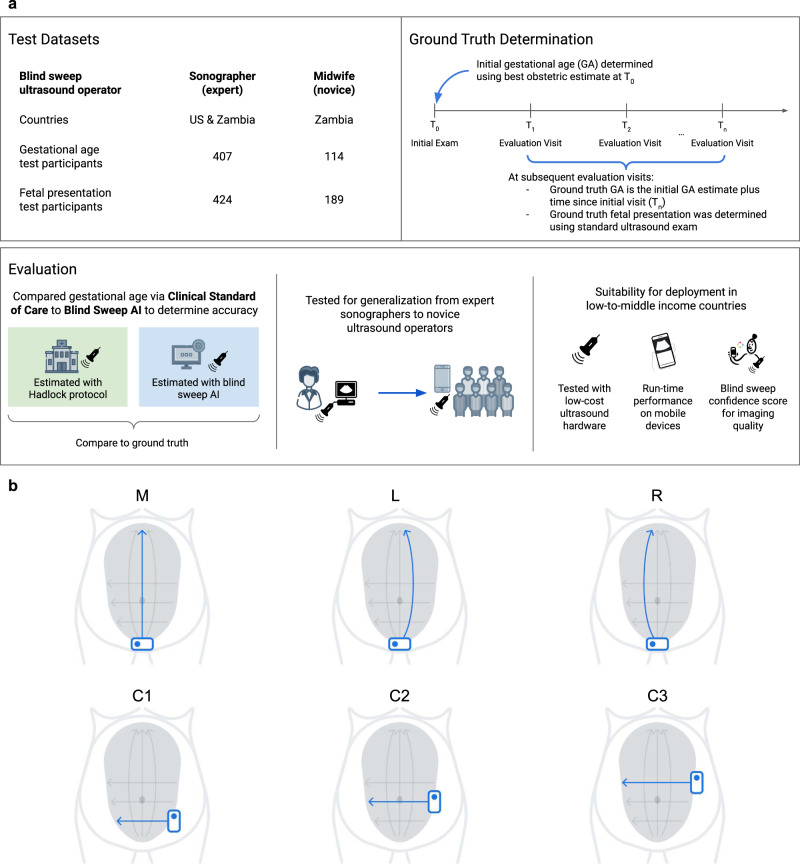
Background: Fetal ultrasound is an important component of antenatal care, but shortage of adequately trained healthcare workers has limited its adoption in low-to-middle-income countries. This study investigated the use of artificial intelligence for fetal ultrasound in under-resourced settings.
Methods: Blind sweep ultrasounds, consisting of six freehand ultrasound sweeps, were collected by sonographers in the USA and Zambia, and novice operators in Zambia. We developed artificial intelligence (AI) models that used blind sweeps to predict gestational age (GA) and fetal malpresentation. AI GA estimates and standard fetal biometry estimates were compared to a previously established ground truth, and evaluated for difference in absolute error. Fetal malpresentation (non-cephalic vs cephalic) was compared to sonographer assessment. On-device AI model run-times were benchmarked on Android mobile phones.
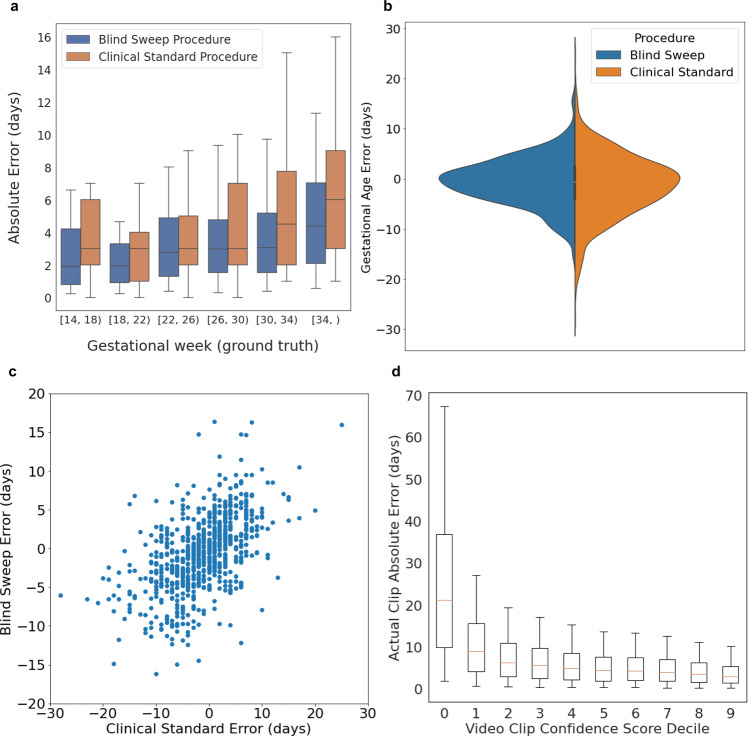
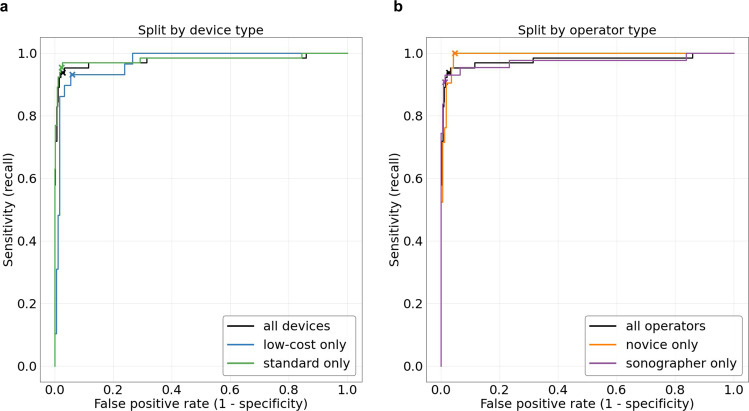
Results: Here we show that GA estimation accuracy of the AI model is non-inferior to standard fetal biometry estimates (error difference -1.4 ± 4.5 days, 95% CI -1.8, -0.9, n = 406). Non-inferiority is maintained when blind sweeps are acquired by novice operators performing only two of six sweep motion types. Fetal malpresentation AUC-ROC is 0.977 (95% CI, 0.949, 1.00, n = 613), sonographers and novices have similar AUC-ROC. Software run-times on mobile phones for both diagnostic models are less than 3 s after completion of a sweep.
Conclusions: The gestational age model is non-inferior to the clinical standard and the fetal malpresentation model has high AUC-ROCs across operators and devices. Our AI models are able to run on-device, without internet connectivity, and provide feedback scores to assist in upleveling the capabilities of lightly trained ultrasound operators in low resource settings.
Keywords: Health care; Medical research.
© The Author(s) 2022.
Conflict of interest statement
Competing interestsThe authors declare the following competing interests: this study was partially funded by Google Inc. R.G.G., C. Lee, A.W., M.S., J.A.T., S.M.M., C.C., S.S., D.T., A.U., K.C., J.G., G.E.D., T. Sp., T. Sa., K.L., T.T., G.C., L.P., J.W., and R.P. are employees of Google Inc. and own stock as part of the standard employee compensation package. The remaining authors declare no competing interests.
Figures
References
-
- World Health Organization. Newborns: improving survival and well-being. https://www.who.int/news-room/fact-sheets/detail/newborns-reducing-morta... (2020).
-
- World Health Organization. Maternal mortality. https://www.who.int/news-room/fact-sheets/detail/maternal-mortality (2019).
-
- Organization, W. H. Strategies Towards Ending Preventable Maternal Mortality (EPMM) (World Health Organization, 2015).
LinkOut - more resources
Full Text Sources
