

Decreasing Inappropriate Telemetry Use via Nursing-Driven Checklist and Electronic Health Record Order Set
- PMID: 36249623
- PMCID: PMC9550181
- DOI: 10.7759/cureus.28999
Decreasing Inappropriate Telemetry Use via Nursing-Driven Checklist and Electronic Health Record Order Set
Abstract
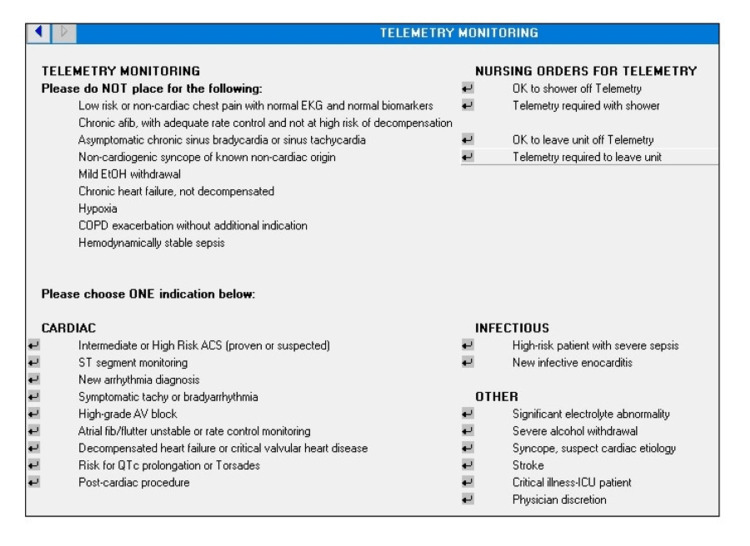
Introduction: Telemetry is ubiquitous in many hospitals despite widely acknowledged limitations, waste, and potential harm associated with inappropriate use. To curb overuse, guidelines such as the 2017 American Heart Association/American College of Cardiology (AHA/ACC) continuous telemetry monitoring practice standards have outlined appropriate telemetry use standards. This study aimed to perform two "plan-do-study-act" (PDSA) cycles and assess whether a nursing (RN)-driven checklist addressing appropriate telemetry use, combined with just-in-time education delivered via an electronic health record (EHR) order set modification, was efficacious in reducing inappropriate telemetry use within a level 1a Veterans Health Administration hospital.
Methods: This is a quality improvement intervention study that took place between March 2019 and August 2020. Three cohorts were sequentially studied: a control cohort without any intervention (n = 100), a cohort with only the RN-driven checklist (n = 100), and a cohort with both the RN-driven checklist and an EHR order set modification that provided just-in-time education about telemetry indications (n = 100). Telemetry records were reviewed by a physician to determine indication, duration for each telemetry order, and appropriateness. An order was deemed "appropriate" if it met AHA/ACC classification grade I (telemetry recommended) or IIa/b (telemetry may be considered) and "inappropriate" if it fell under class III (telemetry not recommended). Data were compared between the control cohort and the two intervention cohorts, as well as between intervention cohorts, using Pearson chi-square analysis. A p-value < 0.05 was considered statistically significant.
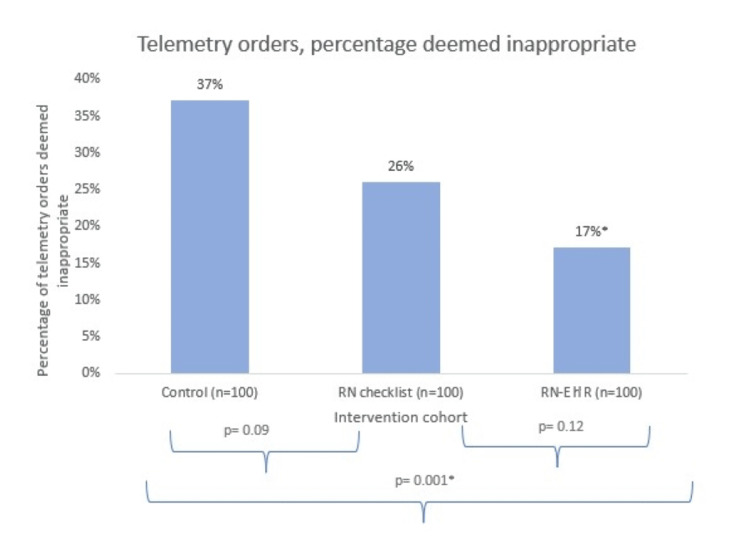
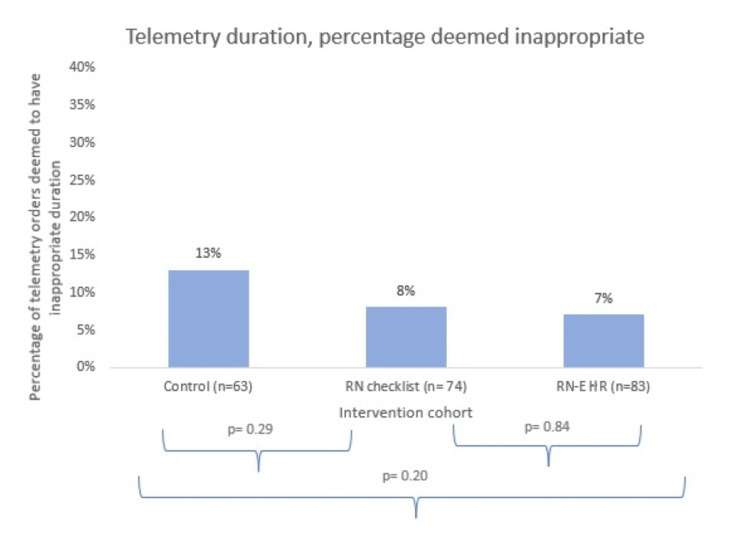
Results: Within the control group, 37% of telemetry orders were deemed inappropriate. After implementation of the RN checklist, a non-statistically significant lower proportion (26%) of orders was deemed inappropriate (p = 0.09). Implementation of the RN checklist, along with the EHR order set, was associated with a significantly lower proportion of inappropriate orders (17%) in comparison to the control cohort (p = 0.001) but not in comparison to the RN checklist cohort (p = 0.12). There was no significant difference in the duration of telemetry use across cohorts.
Conclusions: An RN-driven checklist and EHR telemetry order set modification were associated with a decrease in inappropriate telemetry use from 37% to 17%. By prompting the review of telemetry orders via a daily nursing checklist reviewed during bedside interdisciplinary rounds, clinicians received reinforcement regarding appropriate telemetry indications. This education was strengthened by the just-in-time training provided via the EHR order set.
Keywords: electronic health record (ehr); nursing checklist; patient safety; pdsa cycle; plan do study act; quality improvement; telemetry overuse.
Copyright © 2022, Knees et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Cost-saving opportunities with appropriate utilization of cardiac telemetry. Chong-Yik R, Bennett AL, Milani RV, Morin DP. Am J Cardiol. 2018;122:1570–1573. - PubMed
-
- Eliminating inappropriate telemetry monitoring: an evidence-based implementation guide. Yeow RY, Strohbehn GW, Kagan CM, et al. JAMA Intern Med. 2018;178:971–978. - PubMed
-
- Is telemetry overused? Is it as helpful as thought? Henriques-Forsythe MN, Ivonye CC, Jamched U, Kamuguisha LK, Olejeme KA, Onwuanyi AE. Cleve Clin J Med. 2009;76:368–372. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous