

Impact of Point-of-Care Testing on the Management of Sexually Transmitted Infections in South Africa: Evidence from the HVTN702 Human Immunodeficiency Virus Vaccine Trial
- PMID: 36250382
- PMCID: PMC7614294
- DOI: 10.1093/cid/ciac824
Impact of Point-of-Care Testing on the Management of Sexually Transmitted Infections in South Africa: Evidence from the HVTN702 Human Immunodeficiency Virus Vaccine Trial
Erratum in
-
Correction to: Impact of Point-of-Care Testing on the Management of Sexually Transmitted Infections in South Africa: Evidence from the HVTN702 Human Immunodeficiency Virus Vaccine Trial.Clin Infect Dis. 2023 Jan 6;76(1):182. doi: 10.1093/cid/ciac898. Clin Infect Dis. 2023. PMID: 36450653 Free PMC article. No abstract available.
Abstract
Background: Alternative approaches to syndromic management are needed to reduce rates of sexually transmitted infections (STIs) in resource-limited settings. We investigated the impact of point-of-care (POC) versus central laboratory-based testing on STI treatment initiation and STI adverse event (STI-AE) reporting.
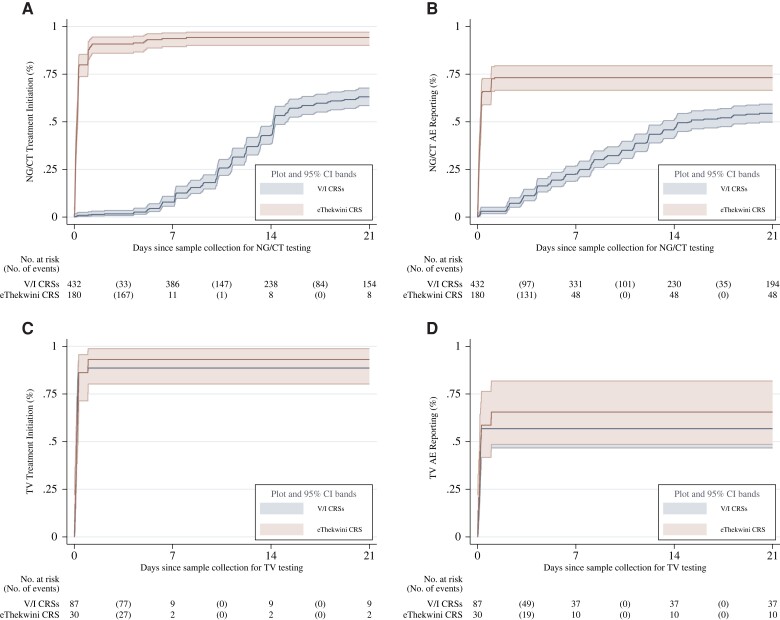
Methods: We used Kaplan-Meier and Cox regression models to compare times to treatment initiation and STI-AE reporting among HVTN702 trial participants in South Africa. Neisseria gonorrhoeae (NG) and Chlamydia trachomatis (CT) were diagnosed POC at eThekwini clinic and in a central laboratory at Verulam/Isipingo clinics. All clinics used POC assays for Trichomonas vaginalis (TV) testing.
Results: Among 959 women (median age, 23 [interquartile range, 21-26] years), median days (95% confidence interval [95%CI]) to NG/CT treatment initiation and NG/CT-AE reporting were 0.20 (.16-.25) and 0.24 (.19-.27) at eThekwini versus 14.22 (14.12-15.09) and 15.12 (13.22-21.24) at Verulam/Isipingo (all P < .001). Median days (95%CI) to TV treatment initiation and TV-AE reporting were 0.17 (.12-.27) and 0.25 (.20-.99) at eThekwini versus 0.18 (.15-.2) and 0.24 (.15-.99) at Verulam/Isipingo (all P > .05). Cox regression analysis revealed that NG/CT treatment initiation (adjusted hazard ratio [aHR], 39.62 [95%CI, 15.13-103.74]) and NG/CT-AE reporting (aHR, 3.38 [95%CI, 2.23-5.13]) occurred faster at eThekwini versus Verulam/Isipingo, while times to TV treatment initiation (aHR, 0.93 [95%CI, .59-1.48]) and TV-AE reporting (aHR, 1.38 [95%CI, .86-2.21]) were similar.
Conclusions: POC testing led to prompt STI management with potential therapeutic and prevention benefits, highlighting its utility as a diagnostic tool in resource-limited settings.
Keywords: adverse event reporting; central laboratory–based testing; point-of-care testing; sexually transmitted infections; treatment initiation.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. S. S. A. K. reports grants or contracts from the NIH (1U54TW012041 and 2UM1AI069469, paid to institution), the South African Medical Research Council (cooperative agreement paid to institution), the National Research Foundation/Department of Science and Technology (UID 96354, paid to institution), the US Agency for International Development/Right to Care (cooperative agreement 72067418CA00029, paid to institution), IQRAA Trust (paid to institution), and European and Developing Countries Clinical Trials Partnership (RIA2017S-2008, paid to institution); received honoraria for participation in the Sanofi medical advisory committee on COVID-19 vaccines (paid to institution); and is a member of the World Health Organization science council (unpaid participation), a member of the BMFG scientific advisory committee (meeting honorarium paid to author), and Vice-President of the International Science Council (unpaid participation). G. G. reports grants from NIH, and funding and support for attending meetings and/or travel from HVTN. J. D. is co–principal investigator of the PHILA and POwER trials of point-of-care HIV viral load testing; Cepheid provided GeneXpert platforms and HIV-1 viral load cartridges for these studies at no cost. A. T. reports a grant from the UK Global Challenge Research Fund (MR/T029803/1, paid to institution). All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- World Health Organization . Guidelines for the management of sexually transmitted infections. Available at: https://apps.who.int/iris/bitstream/handle/10665/42782/9241546263_eng.pd.... Accessed 23 June 2022.
-
- Centers for Disease Control and Prevention . Detailed STD facts—gonorrhea. Available at: https://www.cdc.gov/std/gonorrhea/stdfact-gonorrhea-detailed.htm. Accessed 23 June 2022.
-
- Centers for Disease Control and Prevention . Detailed STD facts—chlamydia. Available at: https://www.cdc.gov/std/chlamydia/stdfact-chlamydia-detailed.htm. Accessed 23 June 2022.
-
- Centers for Disease Control and Prevention . Trichomoniasis—CDC fact sheet. Available at: https://www.cdc.gov/std/trichomonas/stdfact-trichomoniasis.htm. Accessed 23 June 2022.
-
- World Health Organization (WHO) . Global health sector strategy on sexually transmitted infections 2016–2021. Geneva, Switzerland: WHO, 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
