

IL-1β-dependent extravasation of preexisting lung-restricted autoantibodies during lung transplantation activates complement and mediates primary graft dysfunction
- PMID: 36250462
- PMCID: PMC9566897
- DOI: 10.1172/JCI157975
IL-1β-dependent extravasation of preexisting lung-restricted autoantibodies during lung transplantation activates complement and mediates primary graft dysfunction
Abstract
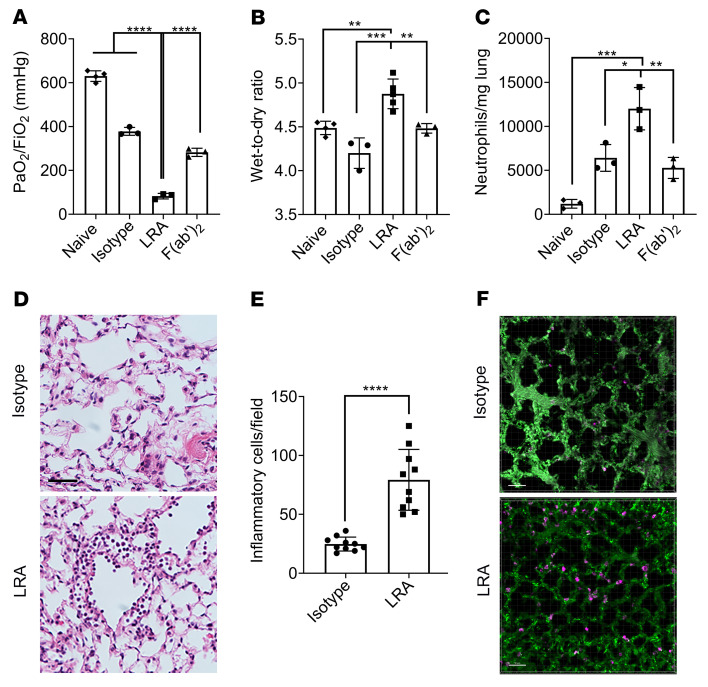
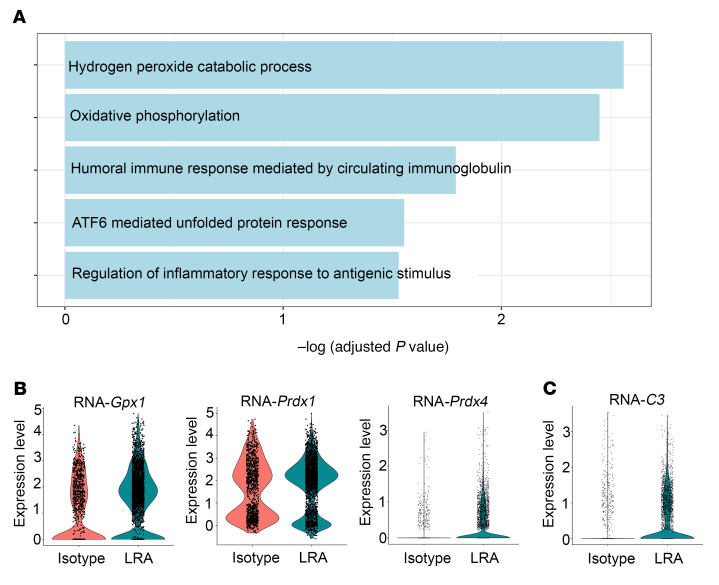
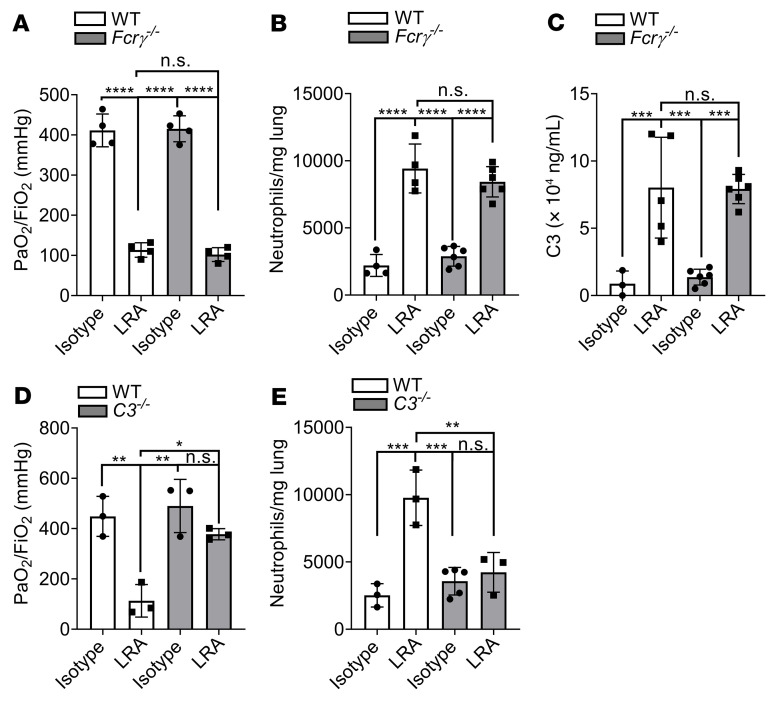
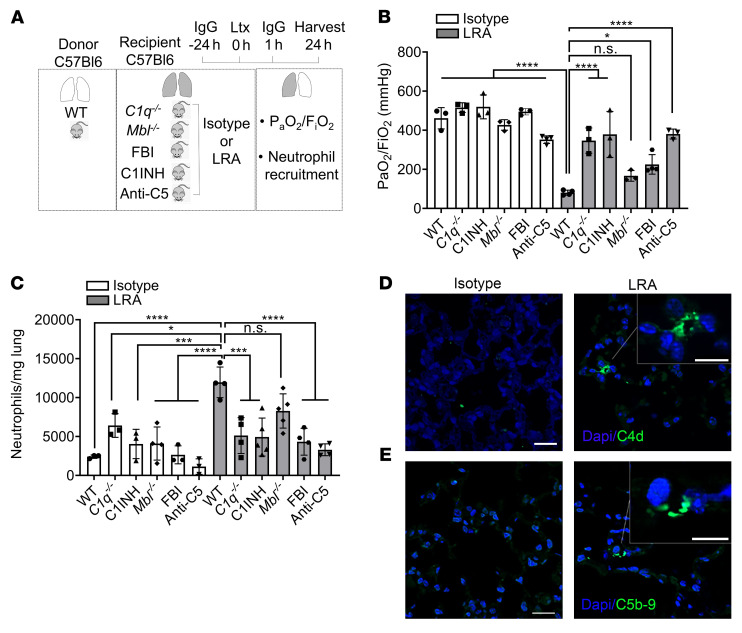
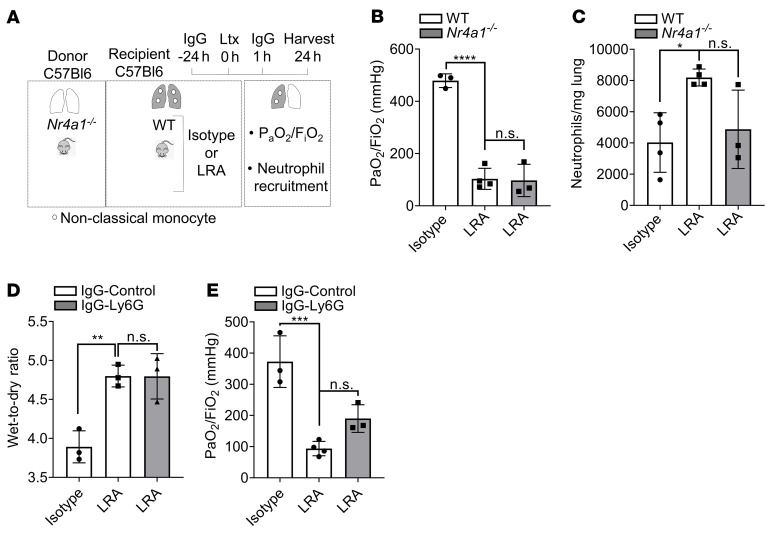
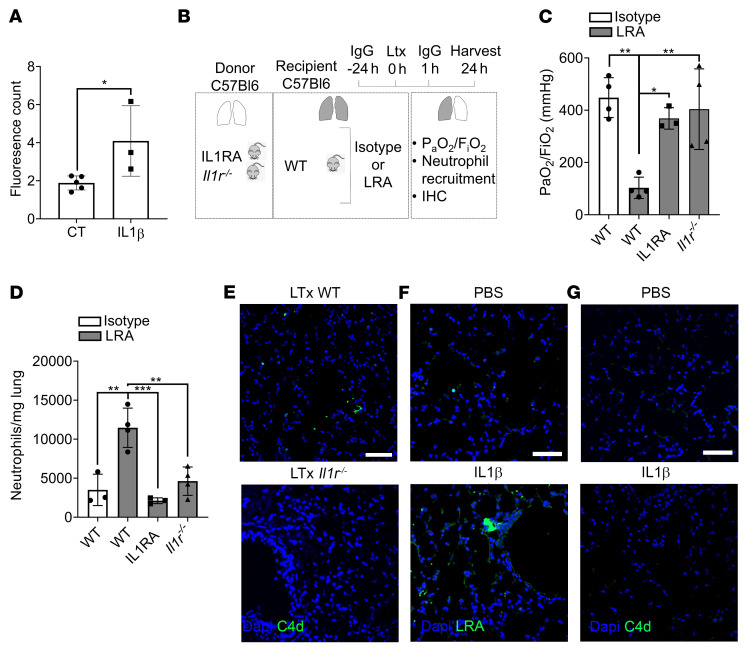
Preexisting lung-restricted autoantibodies (LRAs) are associated with a higher incidence of primary graft dysfunction (PGD), although it remains unclear whether LRAs can drive its pathogenesis. In syngeneic murine left lung transplant recipients, preexisting LRAs worsened graft dysfunction, which was evident by impaired gas exchange, increased pulmonary edema, and activation of damage-associated pathways in lung epithelial cells. LRA-mediated injury was distinct from ischemia-reperfusion injury since deletion of donor nonclassical monocytes and host neutrophils could not prevent graft dysfunction in LRA-pretreated recipients. Whole LRA IgG molecules were necessary for lung injury, which was mediated by the classical and alternative complement pathways and reversed by complement inhibition. However, deletion of Fc receptors in donor macrophages or mannose-binding lectin in recipient mice failed to rescue lung function. LRA-mediated injury was localized to the transplanted lung and dependent on IL-1β-mediated permeabilization of pulmonary vascular endothelium, which allowed extravasation of antibodies. Genetic deletion or pharmacological inhibition of IL-1R in the donor lungs prevented LRA-induced graft injury. In humans, preexisting LRAs were an independent risk factor for severe PGD and could be treated with plasmapheresis and complement blockade. We conclude that preexisting LRAs can compound ischemia-reperfusion injury to worsen PGD for which complement inhibition may be effective.
Keywords: Innate immunity; Organ transplantation; Transplantation.
Figures
Similar articles
-
Crosstalk between nonclassical monocytes and alveolar macrophages mediates transplant ischemia-reperfusion injury through classical monocyte recruitment.JCI Insight. 2021 Mar 22;6(6):e147282. doi: 10.1172/jci.insight.147282. JCI Insight. 2021. PMID: 33621212 Free PMC article.
-
Prolonged Cold Ischemia Induces Necroptotic Cell Death in Ischemia-Reperfusion Injury and Contributes to Primary Graft Dysfunction after Lung Transplantation.Am J Respir Cell Mol Biol. 2019 Aug;61(2):244-256. doi: 10.1165/rcmb.2018-0207OC. Am J Respir Cell Mol Biol. 2019. PMID: 30742487 Free PMC article.
-
CD11b suppresses TLR activation of nonclassical monocytes to reduce primary graft dysfunction after lung transplantation.J Clin Invest. 2022 Jul 15;132(14):e157262. doi: 10.1172/JCI157262. J Clin Invest. 2022. PMID: 35838047 Free PMC article.
-
Primary Graft Dysfunction in Lung Transplantation: An Overview of the Molecular Mechanisms.Int J Mol Sci. 2025 Jul 15;26(14):6776. doi: 10.3390/ijms26146776. Int J Mol Sci. 2025. PMID: 40725023 Free PMC article. Review.
-
Update on the immunological mechanisms of primary graft dysfunction and chronic lung allograft dysfunction.Curr Opin Organ Transplant. 2024 Dec 1;29(6):412-419. doi: 10.1097/MOT.0000000000001175. Epub 2024 Oct 16. Curr Opin Organ Transplant. 2024. PMID: 39422603 Review.
Cited by
-
The role of lung-restricted autoantibodies in the development of primary and chronic graft dysfunction.Front Transplant. 2023 Nov 9;2:1237671. doi: 10.3389/frtra.2023.1237671. eCollection 2023. Front Transplant. 2023. PMID: 38993924 Free PMC article. Review.
-
Contrasting predictors of severe primary graft dysfunction following transplant for chronic and acute respiratory failure.J Thorac Dis. 2024 Aug 31;16(8):5050-5062. doi: 10.21037/jtd-24-100. Epub 2024 Aug 28. J Thorac Dis. 2024. PMID: 39268121 Free PMC article.
-
The HNRNPC/CELF2 signaling pathway drives glycolytic reprogramming and mitochondrial dysfunction in drug-resistant acute myeloid leukemia.Cell Biosci. 2025 May 16;15(1):61. doi: 10.1186/s13578-025-01386-x. Cell Biosci. 2025. PMID: 40380235 Free PMC article.
-
Biomarkers for primary graft dysfunction after lung transplantation: a review of current evidence and future prospects.Front Physiol. 2025 May 22;16:1557182. doi: 10.3389/fphys.2025.1557182. eCollection 2025. Front Physiol. 2025. PMID: 40476215 Free PMC article. Review.
-
B cells mediate lung ischemia/reperfusion injury by recruiting classical monocytes via synergistic B cell receptor/TLR4 signaling.J Clin Invest. 2024 Jan 23;134(6):e170118. doi: 10.1172/JCI170118. J Clin Invest. 2024. PMID: 38488011 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
